45
Aminoglycosides & Spectinomycin
CASE STUDY
A 45-year-old man with no medical history was admitted to the intensive care unit (ICU) 10 days ago after suffering third-degree burns over 40% of his body. He had been relatively stable until the last 24 hours. Now he is febrile (39.5°C [103.1°F]), and his white blood cell count has risen from 8500 to 20,000/mm3. He has also had an episode of hypotension (86/50 mm Hg) that responded to a fluid bolus. Blood cultures were obtained at the time of his fever and results are pending. The ICU attending physician is concerned about sepsis and decides to treat with empiric combination therapy directed against Pseudomonas. The combination therapy includes tobramycin. The patient weighs 70 kg (154 lb) and has an estimated creatinine clearance of 90 mL/min. How should tobramycin be dosed using once-daily and conventional dosing strategies? How should each regimen be monitored for efficacy and toxicity?
The drugs described in this chapter are bactericidal inhibitors of protein synthesis that interfere with ribosomal function. These agents are useful mainly against aerobic gram-negative microorganisms.
 AMINOGLYCOSIDES
AMINOGLYCOSIDES
The aminoglycosides include streptomycin, neomycin, kanamycin, amikacin, gentamicin, tobramycin, sisomicin, netilmicin, and others. They are used most widely in combination with a β-lactam antibiotic in serious infections with gram-negative bacteria, in combination with vancomycin or a β-lactam antibiotic for gram-positive endocarditis, and for treatment of tuberculosis.
General Properties of Aminoglycosides
A. Physical and Chemical Properties
Aminoglycosides have a hexose ring, either streptidine (in streptomycin) or 2-deoxystreptamine (in other aminoglycosides), to which various amino sugars are attached by glycosidic linkages (Figures 45–1 and 45–2). They are water-soluble, stable in solution, and more active at alkaline than at acid pH.
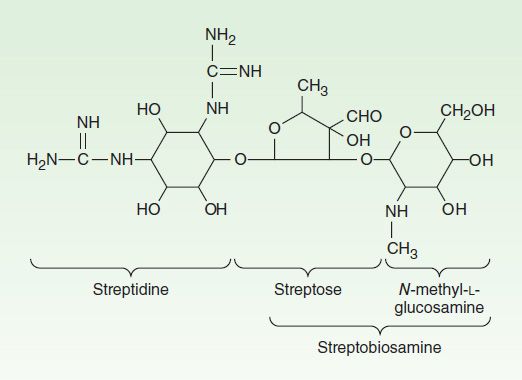
FIGURE 45–1 Structure of streptomycin.
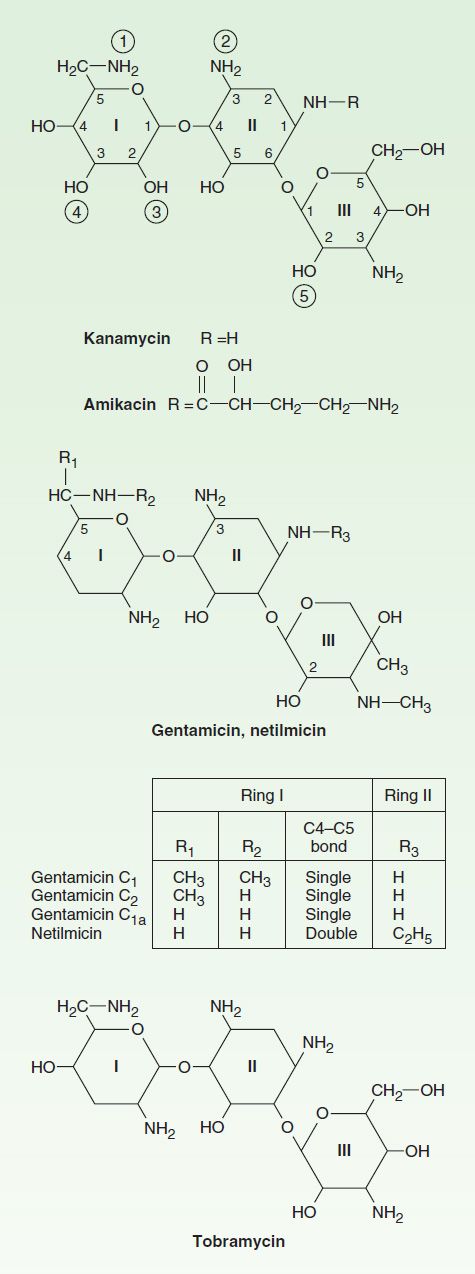
FIGURE 45–2 Structures of several important aminoglycoside antibiotics. Ring II is 2-deoxystreptamine. The resemblance between kanamycin and amikacin and between gentamicin, netilmicin, and tobramycin can be seen. The circled numerals on the kanamycin molecule indicate points of attack of plasmid-mediated bacterial transferase enzymes that can inactivate this drug. ![]() ,
,![]() , and
, and ![]() , acetyltransferase;
, acetyltransferase; ![]() , phosphotransferase;
, phosphotransferase; ![]() , adenylyltransferase. Amikacin is resistant to modification at
, adenylyltransferase. Amikacin is resistant to modification at ![]() ,
, ![]() ,
, ![]() , and
, and ![]() .
.
B. Mechanism of Action
The mode of action of streptomycin has been studied more closely than that of other aminoglycosides, but all aminoglycosides act similarly. Aminoglycosides are irreversible inhibitors of protein synthesis, but the precise mechanism for bactericidal activity is not known. The initial event is passive diffusion via porin channels across the outer membrane (see Figure 43–3). Drug is then actively transported across the cell membrane into the cytoplasm by an oxygen-dependent process. The transmembrane electrochemical gradient supplies the energy for this process, and transport is coupled to a proton pump. Low extracellular pH and anaerobic conditions inhibit transport by reducing the gradient. Transport may be enhanced by cell wall-active drugs such as penicillin or vancomycin; this enhancement may be the basis of the synergism of these antibiotics with aminoglycosides.
Inside the cell, aminoglycosides bind to specific 30S-subunit ribosomal proteins. Protein synthesis is inhibited by aminoglycosides in at least three ways (Figure 45–3): (1) interference with the initiation complex of peptide formation; (2) misreading of mRNA, which causes incorporation of incorrect amino acids into the peptide and results in a nonfunctional protein; and (3) breakup of polysomes into nonfunctional monosomes. These activities occur more or less simultaneously, and the overall effect is irreversible and leads to cell death.
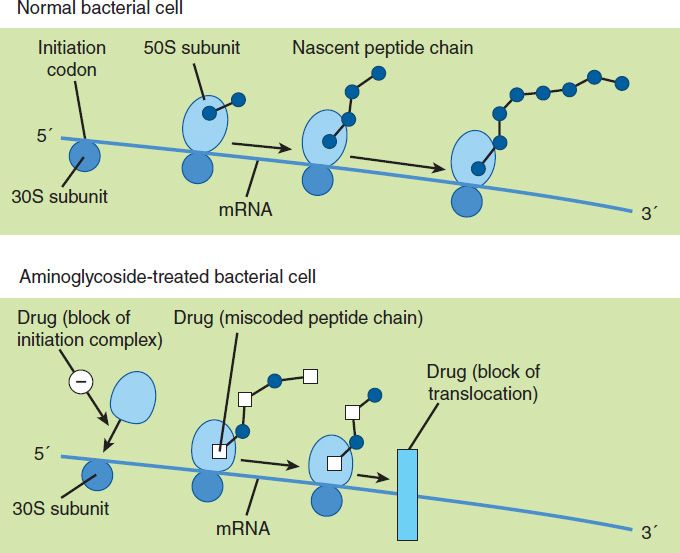
FIGURE 45–3 Putative mechanisms of action of the aminoglycosides in bacteria. Normal protein synthesis is shown in the top panel. At least three aminoglycoside effects have been described, as shown in the bottom panel: block of formation of the initiation complex; miscoding of amino acids in the emerging peptide chain due to misreading of the mRNA; and block of translocation on mRNA. Block of movement of the ribosome may occur after the formation of a single initiation complex, resulting in an mRNA chain with only a single ribosome on it, a so-called monosome. (Reproduced, with permission, from Trevor AT, Katzung BG, Masters SB: Pharmacology: Examination & Board Review, 6th ed. McGraw-Hill, 2002. Copyright © The McGraw-Hill Companies, Inc.)
C. Mechanisms of Resistance
Three principal mechanisms have been established: (1) production of a transferase enzyme or enzymes inactivates the aminoglycoside by adenylylation, acetylation, or phosphorylation. This is the principal type of resistance encountered clinically. (Specific transferase enzymes are discussed below.) (2) There is impaired entry of aminoglycoside into the cell. This may be genotypic, resulting from mutation or deletion of a porin protein or proteins involved in transport and maintenance of the electrochemical gradient; or phenotypic, eg, resulting from growth conditions under which the oxygen-dependent transport process described above is not functional. (3) The receptor protein on the 30S ribosomal subunit may be deleted or altered as a result of a mutation.
D. Pharmacokinetics and Once-Daily Dosing
Aminoglycosides are absorbed very poorly from the intact gastrointestinal tract, and almost the entire oral dose is excreted in feces after oral administration. However, the drugs may be absorbed if ulcerations are present. Aminoglycosides are usually administered intravenously as a 30–60 minute infusion. After intramuscular injection, aminoglycosides are well absorbed, giving peak concentrations in blood within 30–90 minutes. After a brief distribution phase, peak serum concentrations are identical to those following intravenous injection. The normal half-life of aminoglycosides in serum is 2–3 hours, increasing to 24–48 hours in patients with significant impairment of renal function. Aminoglycosides are only partially and irregularly removed by hemodialysis—eg, 40–60% for gentamicin—and even less effectively by peritoneal dialysis. Aminoglycosides are highly polar compounds that do not enter cells readily. They are largely excluded from the central nervous system and the eye. In the presence of active inflammation, however, cerebrospinal fluid levels reach 20% of plasma levels, and in neonatal meningitis, the levels may be higher. Intrathecal or intraventricular injection is required for high levels in cerebrospinal fluid. Even after parenteral administration, concentrations of aminoglycosides are not high in most tissues except the renal cortex. Concentration in most secretions is also modest; in the bile, the level may reach 30% of that in blood. With prolonged therapy, diffusion into pleural or synovial fluid may result in concentrations 50–90% of that of plasma.
Traditionally, aminoglycosides have been administered in two or three equally divided doses per day in patients with normal renal function. However, administration of the entire daily dose in a single injection may be preferred in many clinical situations, for two reasons. Aminoglycosides have concentration-dependent killing; that is, higher concentrations kill a larger proportion of bacteria and at a more rapid rate. They also have a significant postantibiotic effect, such that the antibacterial activity persists beyond the time during which measurable drug is present. The postantibiotic effect of aminoglycosides can last several hours. Because of these properties, a given total amount of aminoglycoside may have better efficacy when administered as a single large dose than when administered as multiple smaller doses.
When administered with a cell wall-active antibiotic (a β lactam or vancomycin), aminoglycosides exhibit synergistic killing against certain bacteria. The effect of the drugs in combination is greater than the anticipated effect of each individual drug, ie, the killing effect of the combination is more than additive. This synergy is important in certain clinical situations, such as endocarditis.
Adverse effects from aminoglycosides are both time- and concentration-dependent. Toxicity is unlikely to occur until a certain threshold concentration is reached, but, once that concentration is achieved, the time beyond this threshold becomes critical. This threshold is not precisely defined, but a trough concentration above 2 mcg/mL is predictive of toxicity. At clinically relevant doses, the total time above this threshold is greater with multiple smaller doses of drug than with a single large dose.
Numerous clinical studies demonstrate that a single daily dose of aminoglycoside is just as effective—and probably less toxic—than multiple smaller doses. Therefore, many authorities now recommend that aminoglycosides be administered as a single daily dose in many clinical situations. However, the efficacy of once-daily aminoglycoside dosing in combination therapy of enterococcal and staphylococcal endocarditis remains to be defined, and the standard lower-dose, thrice-daily administration is still recommended. In contrast, limited data do support once-daily dosing in streptococcal endocarditis. The role of once-daily dosing in pregnancy and in neonates also is not well defined.
Once-daily dosing has potential practical advantages. For example, repeated determinations of serum concentrations are unnecessary unless aminoglycoside is given for more than 3 days. A drug administered once a day rather than three times a day is less labor intensive. And, once-a-day dosing is more feasible for outpatient therapy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


