• When symptomatic: vague feeling of discomfort, pressure, congestion, bloating, heaviness; pain with vaginal sexual activity, urinary frequency, backache, abdominal enlargement, and abnormal bleeding. • Abnormal bleeding occurs in 30% of women with fibroids. • Fibroids can degenerate with necrosis, resulting in cystic de-generation. • Examination by pelvic palpation and/or pelvic ultrasound. • Main diagnostic consideration: differentiating fibroid from ovarian malignant tumor, abscess in fallopian tube/ovarian region, diverticulum of colon, pelvic kidney, endometriosis, adenomyosis, congenital anomalies, or uterine sarcoma. • Uterine fibroids consist of smooth muscle cells and connective tissue. Growth is stimulated by estrogen. They arise during reproductive years, grow during pregnancy, and regress after menopause. Growth spurt can happen in perimenopau-sal years—anovulatory cycles with irregular relative estrogen excess. • Incidence is 20%-25% of women by age 40 years; >50% of women overall; African-American women have higher incidence. Fibroids are the most common indication for major surgery in women and the most common solid tumor in women. • Cause is poorly understood. Factors include increased local estradiol concentration within fibroid itself, higher estrogen receptor density in fibroid tissue than in surrounding myometrium but lower than endometrium. • From 50%-80% of fibroids are asymptomatic. Abnormal bleeding occurs in 30% of women with fibroids (menorrhagia and • Degenerative changes: fibroid outgrows blood supply; cellular detail is lost from decreased vascularity of tumor. Necrosis re-sults in cystic degeneration. Calcification can occur over time, especially in postmenopausal women. • Based on mitotic count, nuclear atypia, and other morphologic features, uterine smooth muscle tumors can be classified as leiomyomas, smooth muscle tumors of uncertain malignant potential, and leiomyosarcomas. • Presumptive diagnosis of fibroids: thorough history and pelvic exam. Palpation findings: enlarged, firm uterus or uterus with irregular edges. • Differentiate possible fibroid from ovarian malignant tumor, fallopian tube or ovarian region abscess, diverticulum, pelvic kidney, endometriosis, congenital anomaly, pelvic adhesions, or rare retroperitoneal tumors. Not all of these can be distinguished by medical history, physical examination, and pelvic ultrasound. Submucosal pedunculated fibroids can be visualized with laparoscopy. Laparoscopy can visualize intramural and subserous fibroids. • Uterine fibroids are classified by location: submucosal (just under endometrium), intramural (within uterine muscle wall), subserosal (from outer wall of uterus), interligamentous (in cervix between the two layers of broad ligament), and pedunculated (on stalk either submucous or subserous). • Natural therapies work best in context of healthy lifestyle and diet. These changes can decrease heavy bleeding or pain and discomfort. • Liver metabolizes estradiol for elimination by converting it to estrone, then to estriol, a weaker estrogen with little influence on the uterus. • Saturated fats, sugar, caffeine, alcohol and junk foods are problematic because they interfere with metabolism of estradiol to estrone to estriol and are deficient in B vitamins or interfere with B-vitamin metabolism. B vitamins facilitate metabolic processes and help regulate estrogen levels. • Whole grains are excellent sources of B vitamins and help excrete estrogens through the bowel. Vegetarian women who eat a high-fiber, low-fat diet have lower blood estrogen than omnivores with low-fiber diets. Fiber may prevent and perhaps reduce fibroids by reducing estrogen influence on uterine tissue. • High-fiber diet may relieve bloating and congestion. Bulking stool and regulating bowel movements may improve bloating. • Uterine fibroids are linked to a fourfold increased risk of endometrial cancer. Three dietary imperatives are to increase fiber, lower dietary fat, and increase soy products and other legumes. Higher fat intake is linked to increased risk for endometrial cancer, higher fiber intake reduces risk for endometrial cancer, and higher soy and legume intake decreases risk of endometrial cancer. • Increase intake of other sources of phytoestrogens (whole grains, vegetables, fruits, seaweeds). • Soy phytoestrogens do not have estrogenic effect on uterus. They are selective of tissues estrogenically affected. In the uterus, soy isoflavones have antiestrogen effect.
Uterine Fibroids
DIAGNOSTIC SUMMARY
GENERAL CONSIDERATIONS
DIAGNOSIS
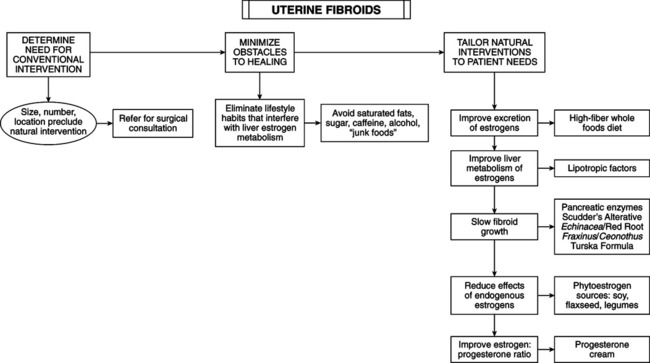
THERAPEUTIC CONSIDERATIONS
Diet
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Uterine Fibroids
