Solid organ transplantation is the optimal mode of therapy for a variety of end-stage diseases, with somewhat variable long-term outcome depending on the organ, as is discussed in this chapter (small bowel, liver, pancreas, kidney, heart, and lung). Kidney and liver transplants are relatively more common; thus, these are presented in greater detail. Although there are many organ-specific features in posttransplantation pathology, there are also many similarities. Postsurgical complications have markedly decreased due to better techniques and donor and recipient management. Immunosuppressive regimens, including multiple drug combinations, are standard of care. Antibody-mediated rejection (AMR) is uncommon, while acute cellular rejection occurs in a majority of recipients and can usually be treated effectively. Chronic rejection is a fibrosing process that continues to be the major limiting factor to long-term survival, and is more frequent in lung and kidney than in heart or liver allografts. These immunocompromised patients are susceptible to both the usual bacterial as well as opportunistic infections, which often involve the lung. Posttransplant lymphoproliferative disease (PTLD), reported to occur in 3% to 5% of recipients, appears to be decreasing even further. It can involve the transplanted organ (rare in heart) as well as extranodal sites such as the gastrointestinal tract.
TRANSPLANT IMMUNOLOGY
Overview
The success of transplantation depends, in large part, on the immune response of the recipient to the donor tissue. The phenomenon of graft rejection was first identified by Peter Medawar in the early 1940s. Medawar and others demonstrated that allogeneic skin grafts (graft from a genetically distinct individual of the same species) would undergo rapid necrosis; however, syngeneic skin grafts (graft from a genetically identical individual) would survive. As almost all solid organ transplants occur between two genetically different individuals (allogeneic graft), many potential foreign or nonself molecules (alloantigens) are available to elicit an immune response and lead to graft failure. Most of these alloantigens are derived from polymorphic genes inherited from both parents and expressed codominantly. One of the most important alloantigens responsible for rejection is encoded by the major histocompatibility complex (MHC). There are three different histopathologic categories of rejection: antibody-mediated (including hyperacute) rejection, acute rejection, and chronic rejection, each of which can also be characterized by immunologic effector mechanisms (humoral versus cell mediated). As transplant immunology is a complex field, only a limited discussion of this broad topic is presented here, and interested readers are referred to many excellent reviews for further reading (1,2).
Antibody-Mediated Rejection
The most severe form of AMR is hyperacute rejection, which is characterized by thrombotic occlusion of the graft vasculature that begins within minutes to hours after blood vessel anastomosis. The mechanism involves preformed antibodies present in the recipient that bind to donor endothelial cells and elicit an immune response characterized by complement activation. Complement proteins are powerful serum proteins that are able to damage cells through either cell lysis or recruitment of inflammatory cells such as neutrophils and macrophages. Classical complement activation occurs when an antibody of the IgM or IgG subclass binds to its cognate antigen and activates C1q. Activation of complement leads to the destruction of donor endothelial cells, resulting in thrombosis. The IgM antibodies responsible for hyperacute rejection are mainly those against the carbohydrate ABO blood group antigen expressed primarily on red blood cells but also on vascular endothelial cells. As most donors and recipients are matched with respect to their ABO subtypes, hyperacute rejection due to anti-ABO antibodies is rare. Although a few centers are successful in performing ABO-incompatible transplantation, it is done only occasionally.
Most forms of AMR occur due to the patient acquiring donor-specific antibodies sometime during the posttransplant period. The incidence is variable depending on the transplanted organ, as detailed in each of the specific sections below.
Acute Allograft Rejection
Acute allograft rejection is commonly encountered in solid organ transplants and has been an area of extensive research. Classically, acute rejection is characterized by the presence of infiltrating lymphocytes that mediate direct killing, macrophage activation, and tissue damage. The lymphocytes involved in this process include CD4+ T-cells, CD8+ T-cells, natural killer (NK) cells, and B cells. Much of transplant immunology has been focused on the role of T cells in rejection, as they are the principal mediators of acute rejection. Indeed, much of the immunosuppressive therapies in use today are directed toward interfering with T-cell function. The mechanism underlying T-cell activation is complex and involves direct presentation of alloantigens (non-self-MHC molecules) to recipient T-cells by donor-derived leukocytes and indirect presentation of alloantigens to recipient T-cells by recipient leukocytes. The process by which recipient T-cells can be directly activated by non-self-MHC molecules on donor cells is still a mystery to most immunologists. During T-cell development in the thymus, those cells, with T-cell receptors, with high affinity for self-MHC molecules are deleted and only those with low affinity for self-MHC survive, thus preventing nonspecific T-cell activation (negative selection) (3). However, in the transplant setting, recipient peripheral T-cells are exposed to non-self-MHC. Immunologists hypothesize that since T-cells with high affinity for these MHC molecules were not deleted by negative selection, there will be a significant proportion (up to 1%) of circulating recipient T-cells with high affinity for non-self-MHC (4). These T-cells could become activated and mediate allograft rejection. The subsequent secretion of cytokines leads to macrophage, neutrophil, and NK cell recruitment (through chemokine and adhesion molecule expression) and tissue destruction (through reactive oxygen species, arachidonic acid metabolites, thrombosis, etc.). In addition, through direct allorecognition, donor CD8+ T-cells can mediate killing. Direct allorecognition is thought to be the principle mechanism by which cellular rejection is mediated.
Indirect recognition of alloantigens is much better understood immunologically as it mirrors what occurs during infections. In this pathway, recipient antigen-presenting cells (dendritic cells and macrophages) phagocytose donor antigens and process them into peptides for presentation on class I and class II MHC. T-cells specific for these peptide: MHC complexes then can become activated and mediate rejection. The proportion of T-cells that would be activated in such a manner is much smaller than in direct allorecognition, and for many years, the significance of this pathway of T-cell activation has been unclear. Recently, indirect presentation has gained the interest of transplant immunologists as it can on its own mediate rejection (5). Moreover, indirect presentation is essential in producing highly specific antidonor antibodies (6). The donor-specific antibodies are mainly directed against donor MHC, both class I and class II. Once formed, these antibodies can bind to donor leukocytes and activated endothelial cells (anti-MHC class II) or all donor cells (anti-MHC class I) resulting in tissue damage through activation of complement and recruitment of inflammatory cells. Indeed, the use of C4d, a product of the complement cascade, as a surrogate of antibody-mediated complement activation has helped pathologists recognize acute humoral rejection (7,8).
Chronic Allograft Rejection
Histologically, chronic rejection in most organs is characterized by fibrosis and vascular damage, and immunologically, this process most likely represents repeated bouts of acute rejection (sometimes subclinical). Thus, both cell-mediated and humoral mechanisms most likely contribute to chronic rejection. Upon activation, some T cells can differentiate into effector cells that produce fibrosing cytokines (9) resulting in collagen deposition and parenchymal extinction. In addition, other cytokines such as platelet-derived growth factor and basic fibroblast growth factor can induce proliferation of smooth muscle cells leading to narrowing of the graft vessels. Moreover, antidonor antibodies have been shown to activate endothelial proliferation and vascular remodeling in animal models (6). The resulting ischemia further leads to parenchymal loss and graft dysfunction. Other causes of late graft dysfunction might not necessarily be related to immunemediated rejection. Indeed, systemic disease such as diabetes, hyperlipidemia, viral infections, etc. can all contribute to late graft dysfunction and should be differentiated from chronic rejection.
Allograft Tolerance
Understanding the immunologic mechanisms of allograft rejection has been essential in developing new therapies as well as defining new histopathologic entities (acute humoral rejection); however, many questions remain. One of the most active fields in transplant immunology is uncovering the mechanisms behind allograft tolerance. The goal of such research is to determine which patients can be removed from immunosuppressive therapy due to tolerance toward the donor allograft. This is particularly important in the pediatric population as immunosuppressive therapy is a major cause of morbidity and mortality. To date, no serologic or histopathologic data can accurately predict graft survival upon withdrawal of medications; however, evidence points to a role of donor-derived leukocytes in mediating allograft tolerance. It is hypothesized that patients who become microchimeras are more likely to become tolerant to their allografts (10). This finding is supported by the early observations that solid organ allografts are accepted to a great extent in individuals who are also receiving partial bone marrow transplants (11). In addition, the greater acceptance of liver allografts is thought to be due to the large number of donor-derived leukocytes present in this organ, some of which may be pluripotent stem cells that can migrate to recipient bone marrow and persist. The recent appreciation of regulatory T cells has also shed light on allograft tolerance. Regulatory T cells have been shown to suppress the function of effector T cells, and active research is underway to enhance the activity of regulatory T cells in order to achieve allograft tolerance (12).
TRANSPLANT PATHOLOGY OF THE INTESTINE
Overview
The introduction of improved immunosuppression has led to a rise in small intestinal transplantation that is of particular importance to the pediatric pathologist as many of the disorders requiring transplantation occur in children: intestinal atresia, necrotizing enterocolitis, intestinal volvulus, Crohn disease, gastroschisis, massive resections, Hirschsprung disease, neuronal intestinal dysplasia, neuropathic and myopathic pseudoobstruction, protein-losing enteropathy, and microvillus inclusion disease (13,14,15). When the liver disease is mild, the intestine can be transplanted in isolation. Signs of portal hypertension and cirrhosis mandate intestinal transplantation in combination with the liver or as part of a multivisceral organ transplant. Indeed, patients receiving combined intestinal/liver transplantation or a multivisceral organ transplant experience fewer episodes of acute rejection and improved overall survival at 5 years (16). Currently, the major obstacle to intestinal transplantation is the availability of appropriate grafts. In particular, size matching is of extreme importance as many pediatric patients have contracted abdominal cavities as a result of previous surgeries.
The pathologist’s role in intestinal transplantation is to evaluate mucosal biopsies in patients with graft dysfunction or as part of a surveillance program. Most institutions routinely take protocol biopsies for the first few months and when clinically indicated thereafter. In evaluating mucosal biopsies, the pathologist must correlate histologic findings with the clinical and endoscopic findings. As with most transplant specimens, a systematic approach evaluating the overall architecture, surface and crypt epithelium, inflammatory infiltrate, and vasculature can prevent pitfalls in diagnosis.
Preservation Injury and Hyperacute Rejection
Due to the intestinal villous circulation, the regenerative compartment of the epithelium is protected from ischemia; thus, preservation injury is less worrisome than in other solid organs. Biopsies taken prior to transplantation demonstrate lamina propria edema and separation of the epithelium from the basement membrane. Shortly after reperfusion, numerous mitoses can be seen within the regenerative compartment along with capillary congestion, villous blunting, and a mild neutrophilic infiltrate (17). Biopsies taken a week after transplantation usually show normal histology even when earlier epithelial damage was quite severe. Hyperacute (antibody-mediated) rejection in small bowel transplants has recently been described, and there is some overlap with preservation injury; however, distinction between the two is usually not difficult. In instances of hyperacute rejection, there is a positive cross-match indicating preformed donor-specific antibodies. These antibodies damage the endothelium leading to fibrin thrombi within the lamina propria vasculature resulting in severe congestion and focal hemorrhage. Neutrophils can be seen marginating within the congested vessels. The presence of fibrin thrombi and severe congestion distinguishes hyperacute rejection from preservation injury (18).
Acute Rejection
Unlike liver allografts, acute rejection is common and remains a major cause of intestinal graft failure. Acute rejection is clinically characterized by nonspecific symptoms such as fever, nausea, vomiting, increased stomal output, abdominal pain, and distention. In severe acute rejection, hemodynamic instability may occur, leading to shock. Endoscopically, acute rejection is characterized by granularity, diminished peristalsis, and, in some cases, mucosal ulceration. Acute rejection can occur at any time in the post-transplant period; however, the first episode of rejection usually occurs within 100 days (14,15). The landmark paper by Lee et al. (17) analyzed the first 62 intestinal transplants performed at the University of Pittsburgh and was the first study to develop histologic criteria for the diagnosis of acute rejection. Subsequent modifications have led to a well-developed histologic grading system for acute rejection that provides a reliable assessment of severity (19).
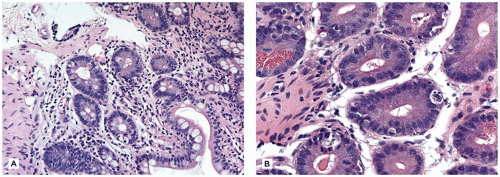
The histologic manifestations of acute rejection include crypt apoptosis, increased lamina propria inflammatory cell infiltrate, and crypt architectural distortion. During most episodes of acute rejection, all biopsies taken from multiple sites will show histologic features of rejection; however, in approximately 20% of cases, only the ileum will be involved. Crypt apoptosis is the earliest histologic sign of rejection, and apoptotic counts should be routinely performed on mucosal biopsy specimens. Rejection is characterized by greater than six apoptotic bodies per ten consecutive crypts, and in mild acute rejection, crypt apoptosis is the dominant histologic feature (Figure 8-1). In addition, mild localized collections of inflammatory cells (predominately activated/blastic lymphocytes with lesser numbers of eosinophils and neutrophils) are present around small venules and capillaries in the deep mucosa. Peyer patches become enlarged and contain large numbers of activated lymphocytes. The crypt epithelium commonly shows features of regeneration including mucin depletion, nuclear enlargement, and hyperchromasia. A mild increase in intraepithelial lymphocytes and occasional neutrophils is typically seen. The villi are shortened, and the crypts may be distorted due to lamina propria expansion.
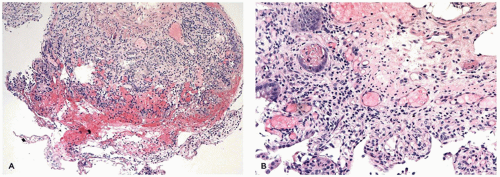
Moderate rejection is characterized by increased crypt apoptotic bodies and a diffuse inflammatory cell infiltrate characterized by activated lymphocytes. Crypt apoptotic bodies begin to appear in the midportions of the crypt and confluent apoptosis in a single crypt may be seen. The villi are flattened to a greater extent; however, extensive ulceration is not common. In severe acute rejection, crypt apoptotic body counts are further increased (up to 20) (Figure 8-2). Mucosal ulcerations are common and, in its place, are fibrinous neutrophilic exudates mimicking pseudomembranous colitis. Care should be taken when evaluating biopsies for acute rejection 100 days post transplant as the inflammatory infiltrate is generally mild and crypt apoptosis is the only dominant histologic feature (17).
FIGURE 8-1 • Mild acute rejection of small bowel allografts. A: The villous architecture is usually preserved, and there is only a mild increase in lamina propria inflammation. B: Prominent apoptotic bodies are the most evident feature (Photos courtesy of Dr. Reetesh Pai, Stanford University).
Chronic Rejection
Chronic rejection in the intestine is less common than in heart, kidney, and lung (20). Patients with chronic rejection have persistent diarrhea despite increased immunosuppressive therapy. Endoscopic and radiographic findings of chronic rejection include loss of mucosal folds, mural thickening, focal ulcers, and decreased arborization of the mesenteric vasculature. Clinically, chronic rejection is encountered late in the posttransplant period, with most cases occurring months after transplantation. There are many factors associated with the development of chronic rejection. Those individuals with acute rejection within 30 days of transplantation and those with severe acute rejection are more likely to develop chronic rejection. Other risk factors include prolonged cold ischemic time, old donor age, and episodes of cytomegalovirus (CMV) infection (20). Simultaneous liver transplantation greatly protects from chronic rejection most likely by decreasing the number of acute rejection episodes. The pathologic process that results in chronic rejection involves arterial obliteration; however, arteries are rarely sampled in endoscopic biopsies. Thus, on mucosal biopsies, one can only suggest possible chronic rejection based on downstream features of chronic ischemia. Early histologic changes that suggest possible chronic rejection include patchy mild fibrosis and focal crypt loss. These nonspecific changes can persist for months. With worsening ischemia due to progression of chronic rejection, there is extensive loss of the intestinal crypts, villous atrophy, mucosal ulceration, and increased lamina propria inflammation and fibrosis. The surviving crypts show evidence of chronic damage including pyloric gland metaplasia (17,20). Once chronic rejection proceeds to the severe stage, the graft is very likely to fail. At resection, the vasculature should be adequately sampled to find the characteristic changes of chronic rejection. In addition, extensive neural hyperplasia is a common finding at resection (21).
FIGURE 8-2 • Severe acute rejection of small bowel allografts. A: Surface ulceration with a prominent lymphocytic infiltrate is common. B: Crypts are typically lost, and the surviving crypts are severely damaged. This differential diagnosis includes ischemia and infection (Photos courtesy of Dr. Reetesh Pai, Stanford University).
Complications of Transplantation
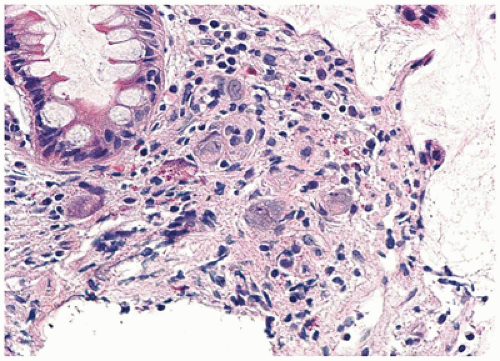
Infection remains a very common complication of transplantation, whether in the postoperative setting or due to immunosuppressive therapies. The majority of infections are bacterial infections although fungal infections are also encountered (15). Of more importance to the pathologist is recognizing viral infections, in particular CMV, Epstein-Barr virus (EBV), and adenovirus. CMV infection is encountered in 5% to 29% of intestinal allograft specimens and can clinically mimic acute rejection (15). Negative CMV serology in the pediatric recipient is associated with increased CMV infection when transplanted with a serologic positive donor (22). In the majority of specimens, a moderate neutrophilic and mononuclear cell infiltrate is seen in the lamina propria as well as in the crypts. Ulceration with abundant granulation tissue can be seen in severe cases. In severely immunocompromised individuals, inflammation may be mild. In addition, crypt atrophy, cell dropout, and apoptotic bodies may be present, mimicking rejection. The characteristic CMV inclusions are mainly confined to the endothelial and stromal cells (Figure 8-3); however, epithelial cells can be infected in severe cases.
FIGURE 8-3 • CMV infection of small bowel allograft. In CMV infection, an inflammatory infiltrate with ulceration, crypt atrophy, and apoptotic bodies can be seen; however, the characteristic cytoplasmic and nuclear inclusions are key in differentiating CMV infection from rejection (Photo courtesy of Dr. Reetesh Pai, Stanford University).
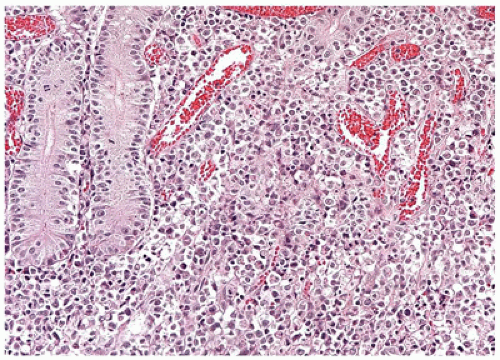
FIGURE 8-4 • Posttransplant lymphoproliferative disorder of small bowel allografts. PTLD is commonly characterized by an atypical inflammatory infiltrate, which can be mixed (polymorphous) as in this case or monomorphic. In situ hybridization for EBER can be helpful in confirming the diagnosis (Photo courtesy of Dr. Reetesh Pai, Stanford University).
Adenovirus is a very common cause of pediatric gastroenteritis; however, until recently, infection of allografts has not been routinely recognized. Pinchoff et al. (23) found a high prevalence of adenoviral infection in pediatric small bowel allografts. Adenoviral enteritis most commonly affects the ileum and is characterized by smudgy epithelial cell nuclear inclusions, epithelial hyperplasia with disarray, and a prominent lymphoplasmacytic infiltrate.
EBV infection is another serious complication in the post-transplant period as it can lead to PTLD (24). EBV infection is associated with a wide histologic spectrum, from simple lymphoid hyperplasia to non-Hodgkin lymphoma. When evaluating a specimen, particular attention should be paid to the type of lymphoid infiltrate (Figure 8-4). If small lymphocytes predominate, one can be reassured; however, the presence of large atypical lymphoid cells should prompt concern for PTLD and in situ hybridization for EBV early RNA (EBER) should be performed. A large number of EBER-positive cells (>15 per high-power field) with a heterogeneous population of lymphoid cells, including immunoblasts, plasma cells, and large cleaved cells, are characteristic of polymorphous PTLD (Figure 8-4) (24). If the lymphoid population is homogenous, the designation of monomorphic PTLD is made, and further classification is made according to established criteria (24). The vast majority of monomorphic PTLDs are B cell in origin; however, T-cell PTLDs have been described.
The Gastrointestinal Tract in Graft Versus Host Disease
The intestinal tract is one of the three major target organs in graft versus host disease (GVHD) (25,26). The skin and the liver are the other two organs affected when donor lymphoid cells are transfused into immunosuppressed host. GVHD usually occurs in the setting of bone marrow transplantation but may also rarely occur following the transfusion of non-irradiated blood into patients with primary or secondary immunodeficiency disorders (27). Conceptually, GVHD mirrors allograft rejection as donor leukocytes recognize recipient tissues as “foreign” and attempt to “reject” them. Thus, the immunologic effector mechanisms are similar.
The gastrointestinal tract is affected in at least half of patients with acute GVHD and classically occurs within the first 100 days posttransplantation; however, persistent, recurrent, or late-onset acute GVHD is a well-recognized phenomenon (25). Intestinal GVHD is usually heralded by profuse watery diarrhea, which indicates involvement of the small intestine and colon. Occasionally, the upper gastrointestinal tract will be involved first or exclusively; the symptoms are nausea, vomiting, and anorexia. Acute intestinal GVHD is usually diagnosed by colonoscopic biopsy or endoscopic biopsy of the upper gastrointestinal tract. The earliest histologic changes occur deep in the crypts (the regenerative compartment) with epithelial infiltration by lymphocytes and subsequent apoptosis of individual glandular cells (28,29) (Figure 8-5). The minimum necessary criteria to diagnose acute GVHD are variable across institutions. At a minimum, more than one apoptotic body per biopsy fragment is necessary to consider a diagnosis of acute GVHD (30). However, in the setting of cytomegaloviral infection, recent chemotherapy, and features suspicious for medication injury, it may not be possible to definitively diagnosis GVHD. If appropriate therapy is not instituted, glandular destruction and ulceration are seen. Complete crypt loss, villous atrophy, and extensive mucosal denudation occur in advanced acute GVHD. In the esophagus, vacuolization and inflammation of the epithelial basal layer with apoptosis of squamous epithelial cells and eventual desquamation and ulceration are seen (31).
Chronic GVHD is a more insidious process that primarily affects the skin and liver. The intestinal tract is largely spared; however, features of chronic injury can be seen (32). In the esophagus, a scleroderma-like fibrosis and dysmotility may develop (33). In the evaluation of all the phases of intestinal GVHD, opportunistic infections must be ruled out (31). Interestingly, mycophenolate mofetil, a commonly used immunosuppressive drug in solid organ transplantation, can give rise to histologic findings similar to acute GVHD (34).
FIGURE 8-5 • GVHD of the small bowel. GVHD is characterized by apoptosis of individual epithelial cells lining the crypts similar to acute rejection seen in small bowel transplants. If severe, complete villous loss and surface ulceration can be seen.
TRANSPLANT PATHOLOGY OF THE LIVER
Overview
In the United States, approximately 10% of the total number of liver transplants occur in the pediatric population (35). The indications for liver transplant are diverse (Table 8-1) (35); the most common continues to be extrahepatic biliary atresia.
TABLE 8-1 INDICATIONS FOR PEDIATRIC LIVER TRANSPLANTATION
Noncholestatic cirrhosis
Autoimmune hepatitis
Chronic viral hepatitis
Cholestatic liver disease/cirrhosis
Caroli disease
Choledochol cyst
Primary sclerosing cholangitis
Biliary atresia
Extrahepatic
Alagille syndrome
Hypoplasia
Acute hepatic necrosis
Acute viral hepatitis
Drugs
Metabolic diseases
Alpha-1-antitrypsin deficiency
Wilson disease
Hemochromatosis
Tyrosinemia
Primary oxalosis
Glycogen storage disease types Ia, Ib, III, and IV
Hyperlipidemia
Urea cycle disorders
Crigler-Najjar syndrome
Malignant neoplasms
Hepatoblastoma
Hepatocellular carcinoma
Other
Cystic fibrosis
Budd-Chiari syndrome
Congenital hepatic fibrosis
TPN/hyperalimentation
Familial cholestasis
Hepatic adenomatosis
Early in pediatric transplantation, the survival rates were dismal as only 30% of patients survived greater than 1 year (13). With improved surgical techniques, patient screening, and immunosuppression, the current 1-year patient survival is 90% and the 5-year survival is 80%. Graft survival is 85% at 1 year and 67% at 5 years (35). The early days of pediatric liver transplantation were also complicated by a shortage of appropriate-sized liver allografts. With the advent of reduced-sized liver transplantation, living-related transplantation, and, most importantly, split-liver transplantation, the shortage of pediatric liver allografts has been somewhat alleviated (13,36,37). In split-liver transplants, the whole adult cadaveric liver is divided into two functional segments: one for adults (right trisegment) and one for children (left lateral segment). Recent studies have shown that split-liver recipients have comparable survival to whole liver recipients (38,39). Despite these improvements, surgical complications continue to be more common when compared with adults (13,36,40). In particular, the use of partial liver allografts predisposes to biliary complications (41). In addition, hepatic artery thrombosis (HAT) is more common in pediatric patients owing to the technically difficult surgery. However, the improvement in surgical techniques and postoperative management has improved, allowing many of these grafts to be saved. Portal vein thrombosis is occasionally encountered, which, in most cases, resolves without need for intervention (40). Hepatic vein thrombosis is rarely encountered except in patients undergoing liver transplantation for Budd-Chiari syndrome. Bowel perforation is common in the pediatric population as most of these patients have had previous abdominal surgery and suffer from poor nutrition. Other complications of liver transplant can be roughly grouped into the time periods in which they are most likely to occur (Table 8-2) (42).
TABLE 8-2 APPROXIMATE TIMELINE OF BIOPSY FINDINGS IN LIVER TRANSPLANTATION
Lymphoplasmacytic infiltrate with interface activity
The initial outcome of the liver allograft depends on the health of the donor liver, the amount of ischemic time the allograft suffered, the presence of preformed antiallograft antibodies, and complications encountered during surgery and the perioperative period. Acute rejection and viral infections tend to occur between 1 week and 2 months post transplantation, whereas chronic rejection and recurrent disease are late manifestations. However, the timing can vary significantly (e.g., late-onset acute rejection), and biopsy interpretation remains essential.
Preservation Injury
Preservation (harvesting) injury results from donor and tissue procurement factors that contribute to poor allograft function in the perioperative period. In order to diagnose preservation injury, one must exclude injury due to surgical complications, immunologic reactions, and drug toxicity. Warm and cold ischemia preferentially damages hepatocytes and endothelial cells, respectively. Endothelial cell damage leads to interference with vascular blood flow and subsequent allograft injury. Many donor factors can increase the susceptibility of the allograft to ischemic time. One of the most studied is the presence of donor macrovesicular steatosis. Transplantation of liver allografts with greater than 50% macrovesicular steatosis, on frozen section analysis, may result in poor graft function as steatotic hepatocytes are sensitive to ischemic damage. Other donor factors that influence graft function include fibrosis, chronic liver disease, hemodynamic instability, infections, donor atherosclerosis, and donor age (43,44).
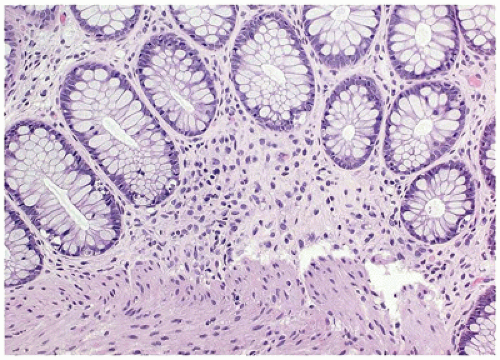
Clinically, preservation injury is characterized by poor bile production and persistent elevations of serum ALT and AST. The histologic features of preservation injury are usually apparent within 1 to 2 days after revascularization. In mild preservation injury, mild centrilobular hepatocyte ballooning and canalicular cholestasis are commonly seen. Occasionally, neutrophils may be present. On low-power microscopic evaluation, preservation injury can be suggested by pallor in the centrilobular areas. The hepatocyte injury is rapidly reversible; however, the cholestasis may persist for several weeks (Figure 8-6). In more severe injury, zonal necrosis and severe neutrophilia may be seen. In these biopsies, bile ductular proliferation as well as cholestasis may be prominent. In patients receiving a steatotic liver, reperfusion results in lysis of the steatotic hepatocytes with formation of sinusoidal fat droplets that disrupt hepatic blood flow. The extracellular fat may persist for weeks after initial injury. Resolution of hepatic injury is the hallmark of preservation injury, but if severe, the allograft may fail resulting in primary nonfunction. If hepatocyte injury persists beyond 1 week, other diagnoses such as rejection and obstructive cholangitis should be considered.
It is our practice to report the percentage of macrovesicular steatotic hepatocytes, the amount of fibrosis, and the presence of perivenular necrosis (45) to our transplant surgeons who ultimately determine allograft use.
Hepatic Artery Thrombosis
As previously mentioned, HAT remains a significant problem in pediatric liver transplantation and is a complication in 5% to 10% of pediatric liver allografts (40). The incidence of HAT increases with decreasing age due to the smaller size of the arterial anastomosis. As the hepatic artery is the sole blood supply to the biliary tree, HAT should be sought whenever a biliary leak is found. HAT can occur early in the posttransplant period or late (occurring >30 days post transplant). Early HAT is associated with severe graft dysfunction and high mortality rate. In early HAT, rapid diagnosis and repair of the vascular tree are essential in reversing biliary damage and prevention of allograft failure. Even with aggressive treatment, retransplantation may be necessary; however, in one study, 40% of children with HAT survived without retransplantation (46).
FIGURE 8-6 • Preservation injury of liver allografts. Pallor in the centrilobular areas with hepatocyte ballooning occurring shortly after transplantation is characteristic of mild preservation injury. Hepatocyte and canalicular cholestasis can also be quite prominent in some cases.
In late HAT, the allograft is less susceptible to damage as collaterals have formed. Indeed, many patients are asymptomatic. Symptomatic patients commonly present with recurrent cholangitis, biliary tract strictures (due to prolonged ischemic damage), abscess, and fever. Biopsy findings in HAT are nonspecific, variable, and irregularly distributed within the graft (42). The earliest histologic features of arterial insufficiency include scattered apoptotic hepatocytes and increase mitotic activity (30). If ischemia persists, coagulative necrosis of the centrilobular hepatocytes is frequently encountered along with bile duct necrosis. In late HAT, features of biliary obstruction are encountered, including canalicular cholestasis, cholate stasis, and bile ductular proliferation. In addition, centrilobular hepatocyte ballooning and dropout are commonly seen. Although these findings suggest HAT, definitive diagnosis requires clinical correlation.
Biliary Complications
In children, biliary tract complications are more numerous due to surgical difficulties and the use of split-liver allografts (36,40,47). Clinically, biliary complications should be suspected when preferential increases in alkaline phosphatase and gamma-glutamyl transferase occur. Minor strictures may be asymptomatic with only minor elevations in biliary enzymes, whereas complete obstruction, cholangitic abscess, and ascending cholangitis result in fever, jaundice, right upper quadrant pain, and bacteremia. In the acute phase, liver biopsies show portal edema, ductular reaction, canalicular cholestasis, and a portal inflammatory cell infiltrate rich in neutrophils that is intimately associated with the proliferating ductules. Chronic obstruction leads to cholate stasis, chronic portal inflammation, focal bile duct loss, and portal fibrosis. Progression to biliary cirrhosis can occur if the obstruction is not relieved. Biliary-vascular fistula is a serious complication that warrants prompt surgical correction. Histologically, bile is found in blood vessels often with a giant cell reaction, and red blood cells are found within bile ducts.
Antibody-Mediated (Humoral) Rejection
The liver is relatively resistant to injury by antidonor antibodies for multiple reasons including clearance of antibodies by resident Kupffer cells, dual blood supply, and large sinusoidal surface area, which facilitates absorption of antibodies (48). Antidonor antibodies may be preformed or develop de novo. Preformed antibodies against ABO blood group antigens can give rise to hyperacute AMR; however, the significance of preformed and de novo antibodies against other antigens, particularly HLA, is less clear.
Hyperacute AMR is suspected first in the operating room when the liver becomes swollen and hard and bile is not produced, soon after revascularization. Hemostasis may be difficult to achieve in these patients. Histologically, hyperacute rejection may be difficult to distinguish from primary nonfunction. In severe cases (mostly those due to ABO incompatibility), there tend to be large areas of infarction, portal vein thrombi, and necrotizing arteritis. With appropriate clinical history, such as positive cross-match and short ischemic time, hyperacute rejection may be suggested.
There is much conflicting literature regarding the significance of donor-specific antibodies in ABO-compatible livers. In this setting, the donor-specific antibodies are often against the HLA complex. Some patients with high levels of donor-specific antibodies may develop liver injury that is characterized by centrilobular hepatocyte ballooning, canalicular cholestasis, scattered acidophil bodies, and bile ductular proliferation. These features may be indistinguishable from preservation injury and biliary outflow impairment. Some biopsies also show features of acute cellular rejection, and these cases may be less responsive to conventional immunosuppression. Unlike cardiac and renal allograft biopsies, immunohistochemistry for C4d has limited diagnostic utility. However, in the setting of donor-specific antibodies, clinical evidence of graft dysfunction, and histologic evidence of graft injury, the presence of diffuse stromal staining for C4d in greater than 50% of portal tracts supports the diagnosis of AMR (49).
Acute Cellular Rejection
Acute rejection is fairly common in pediatric liver allografts. Most episodes occur within the first few months after transplantation and can easily be controlled by traditional immunosuppressive therapy. However, a somewhat distinct form of acute rejection can occur late in the posttransplant period, aptly termed late acute rejection. These rejection episodes tend to be more resistant to standard immunosuppressive therapy and have unique histologic features. Most cases of late acute rejection in children are due to inadequate immunosuppression (50). Clinically, acute rejection can be asymptomatic when mild. More severe cases present with fever, decreased bile flow, and elevations in liver chemistry tests. The gold standard for confirming the diagnosis remains liver biopsy; however, communication between the pathologists and clinician is essential in determining which patients with rejection require increased immunosuppression.
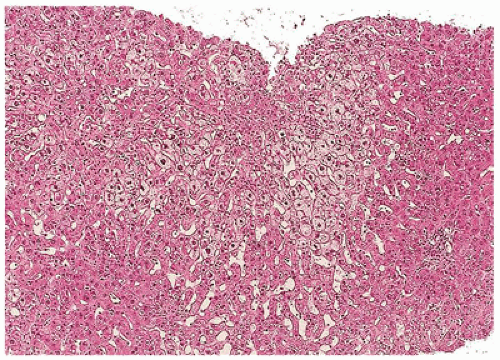
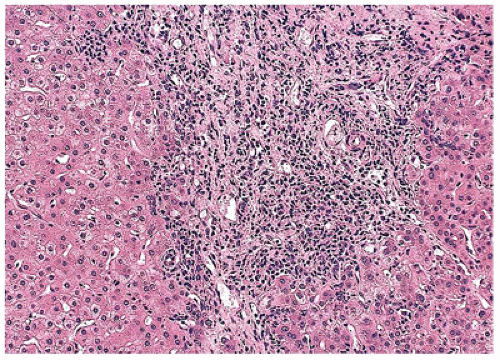
FIGURE 8-7 • Acute rejection of liver allografts. A: The portal tracts in acute rejection are expanded by a dense mixed inflammatory infiltrate. B: Definitive evidence of endothelialitis along with bile duct damage confirms the diagnosis.
In 1997, the Banff working group convened to develop histologic criteria outlining three core histologic features: (a) portal inflammation, (b) subendothelial inflammation, and (c) bile duct damage (51) (Figure 8-7). The portal inflammation is mixed. Activated (blastic) lymphocytes and small mononuclear cells tend to predominate; however, eosinophils, macrophages, and neutrophils can be prominent.
PTLD should be kept in mind when a monotonous portal infiltrate consisting of blastic lymphocytes is present without other features of rejection. The presence of mononuclear inflammatory cells between the endothelial cells of the portal or central vein and the underlying basement membrane, referred to as endothelialitis, is another common feature of rejection. Occasionally, central vein endothelialitis and/or perivenulitis may be the only prominent feature of acute rejection. Bile duct damage is manifested by the presence of mononuclear cells inside the basement membrane and between cholangiocytes. In addition, the bile duct epithelium shows loss of apical cytoplasm (increased nuclear/cytoplasmic ratio), paranuclear vacuolization, nucleoli, nuclear overlap, mitosis, apoptotic bodies, and cytoplasmic eosinophilia. To make a diagnosis of acute rejection, two of three of the above histologic features must be present. The diagnosis is further strengthened if greater than 50% of bile ducts are damaged or if unequivocal endothelialitis is present.
Once the diagnosis of acute rejection is made based on the above criteria, an indication of the global severity should be given. In mild acute rejection, portal inflammation is mild. In moderate rejection, most or all of the portal tracts are expanded by an inflammatory infiltrate. In severe rejection, there is spillover into the hepatic parenchyma with hepatocyte necrosis, both periportal and perivenular. A rejection activity index has been developed to further characterize the severity of rejection and is routinely reported at some institutions (51,52).
As mentioned, late-onset acute rejection has some unique morphologic features when compared with acute rejection occurring early in the posttransplant period (50,53). Late acute rejection tends to have less portal inflammation, increased interface activity, less endothelialitis, and more lobular activity; however, traditional features of acute rejection should still be present. In some cases, only centrilobular pathology exists with perivenular inflammation and zone 3 hepatocyte dropout (isolated central perivenulitis).
Chronic Rejection
Chronic rejection has become relatively rare with current immunosuppressive therapy. Some studies report almost no cases of chronic rejection in pediatric patients (54); however, chronic rejection does occur and is an important cause of late graft failure. Factors associated with chronic rejection include a primary diagnosis of autoimmune liver disease, late-onset acute rejection, nonwhite race, baseline immunosuppression, certain tumor necrosis factor-2 alleles, and CMV infection (controversial) (55,56,57). Despite the name, many cases of chronic rejection occur within months of transplant (2 to 6 months) and lead to graft failure within 2 years. Indeed, unlike other solid organ allografts, chronic rejection in the liver decreases with time, except for a small group of patients with late-onset chronic rejection. The classic presentation of chronic rejection is that of a patient with multiple episodes of acute rejection who develops progressive cholestasis and elevations in alkaline phosphatase, bilirubin, and gamma-glutamyl transferase and is unresponsive to immunosuppressive therapy. Rarely, patients present with chronic rejection in the absence of any documented history of acute rejection.
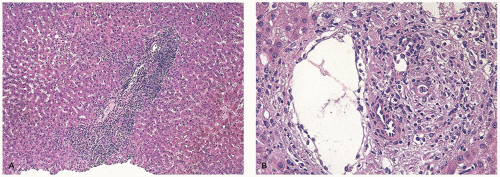
FIGURE 8-8 • Chronic rejection of liver allografts. A: In early chronic rejection, the biliary nuclear/cytoplasmic ratio is increased, and the cytoplasm shows prominent eosinophilia. B: In late chronic rejection, the bile ducts are lost, and only portal veins and, to a lesser extent, terminal hepatic arterioles remain to identify portal tracts. There is an “empty” appearance to the often diminutive portal tracts.
As chronic rejection most commonly results from repeated bouts of acute rejection, there will be a period of overlap. Conceptually, acute rejection refers to reversible and active lesions in which there is hepatocyte apoptosis and blastic portal inflammation, whereas chronic rejection is generally nonreversible and refers to loss of key structures. If both features are present, both acute and chronic rejection should be diagnosed based on their respective criteria. Late clinical findings of chronic rejection include hepatic infarction and loss of synthetic function. Clinically and pathologically, chronic rejection can resemble biliary obstruction and ischemic cholangiopathy.
Like acute rejection, there are three histopathologic features of chronic rejection: (a) bile duct atrophy, (b) foam cell arteriopathy, and (c) bile duct loss, at least one of which should be present (52,58). The diagnosis of chronic rejection mainly depends upon bile duct features as the characteristic foam cell arterial changes are rarely encountered on routine liver biopsies. Thus, it is important to exclude other causes of duct injury or loss such as HAT, obstructive biliary disease, recurrent chronic hepatitis, drug reactions, and CMV infections. The bile duct damage is thought to be ischemic in nature due to damage to the peribiliary arterial plexus. The earliest manifestations of bile duct injury include eosinophilic transformation of the biliary cytoplasm, uneven nuclear spacing, syncytial formation, nuclear enlargement and hyperchromasia, and ducts with focal epithelial cell loss (Figure 8-8A). At this early stage of chronic rejection, it is thought that these changes may be reversible with immunosuppression. In late chronic rejection, bile ducts and, to a lesser extent, terminal hepatic arterioles are lost (Figure 8-8B). When quantifying bile duct and arterial loss, it is essential to remember that in a normal liver, not all portal tracts contain these structures. In fact, between 5% and 10% of portal tracts do not contain bile ducts or hepatic artery branches (59). Thus, bile duct loss is only significant if greater than 20% of the portal tracts do not have bile ducts. However, quantification of bile duct and arterial loss can be complicated in late chronic rejection as portal tracts can be difficult to visualize. In these cases, portal tracts should be inferred from location within the lobule, presence of hepatic arteries, and shape. Additionally, inflammatory cells may obscure bile ducts. In such cases, immunohistochemistry for cytokeratin 7 may be useful in determining bile duct number; however, care must be taken to count only true bile ducts and not ductules (60).
Foam cell arteriopathy is another hallmark of chronic rejection; however, it is best appreciated in large-sized and medium-sized hepatic artery branches that can only be sampled on hepatectomy specimens. Early chronic rejection is characterized by accumulation of foam cells within the intima without luminal compromise. In late rejection, foam cell accumulation with luminal compromise predominates. Changes in large bile ducts can also be appreciated in hepatectomy specimens, including fibrosis of the wall, epithelial sloughing, and papillary hyperplasia. In most cases of chronic rejection, both bile duct loss and foam cell arterial changes coexist; however, up to 15% of cases may have only one feature.
Centrilobular changes can also be seen in chronic rejection and may be a prominent feature. In early chronic rejection, perivenular mononuclear inflammation, hepatocyte dropout, acidophil bodies, pigmented macrophages, and mild fibrosis are commonly seen. Late chronic rejection is characterized by perivenular fibrosis that can be extensive, resulting in bridging fibrosis. Vascular damage due to chronic rejection may be a cause of these centrilobular changes; however, immunologic factors may also contribute to these findings. Centrilobular cholestasis can also be prominent, especially when bile duct loss becomes severe. Many factors not related to chronic rejection may also lead to similar centrilobular changes such as viral hepatitis, venous outflow obstruction, and HAT. Thus, definitive diagnosis of chronic rejection must rely on bile duct and arterial changes.
De Novo and Recurrent Autoimmune Hepatitis
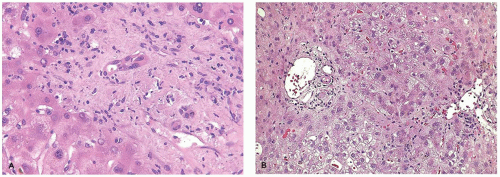
Patients who are transplanted due to autoimmune hepatitis (AIH) can develop recurrent disease (30% by 5 years); however, some patients without any prior history develop a syndrome remarkably similar to classic AIH termed de novo AIH, plasma cell hepatitis, or immune-mediated hepatitis. The diagnosis of de novo or recurrent AIH requires the presence of autoantibodies, lymphoplasmacytic portal inflammation with prominent interface and lobular activity, serologic evidence of liver injury, hypergammaglobulinemia, and no evidence of viral hepatitis, drug-related hepatitis, or rejection (Figure 8-9) (53).
FIGURE 8-9 • De novo autoimmune hepatitis. The portal tract is expanded by a dense lymphoplasmacytic infiltrate with prominent interface and lobular activity. Along with elevated ANA titers, these findings are consistent with a de novo autoimmune hepatitis.
Other Recurrent Diseases
In children, recurrent hepatitis C or B is generally not routinely encountered as chronic viral hepatitis is an uncommon indication of pediatric liver transplantation. In addition, intrinsic metabolic or synthetic liver disease does not recur in the allograft. However, metabolic diseases that secondarily affect the liver can recur in the allograft. These diseases include Niemann-Pick disease, Gaucher disease, cystinosis, and erythropoietic protoporphyria (61).
Recent evidence has confirmed that primary sclerosing cholangitis (PSC) can recur in approximately 5% to 20% of patients with most recurrences diagnosed more than 1 year post transplant (62). Moreover, PSC patients are at a higher risk of developing rejection and worsening inflammatory bowel disease after transplantation. Because in the post-transplant setting there are many causes of biliary disease, the diagnosis of recurrent PSC is often difficult, and no gold standard exists. Thus, close clinical, radiologic, and histopathologic correlation is required to make this diagnosis. The presence of nonanastomotic biliary strictures is suggestive of recurrent PSC but only if occurring late in the posttransplant period. In addition, other causes of late-onset biliary strictures, such as chronic rejection, arterial insufficiency, and biliary infections must be excluded. Early stricturing is more likely due to complications of preservation injury and HAT. Biopsies showing characteristic “onion-skinning” cholangitis or fibro-obliterative changes have been shown to occur only in allografts from PSC patients, but these features are seen only in a small percentage of patients. Thus while specific absence of these features does not rule out recurrent PSC. Features of biliary obstruction are more commonly seen in recurrent PSC; however, these features are nonspecific. Currently, guidelines suggest that recurrent PSC should be suggested in cases with a confirmed diagnosis of PSC before transplant; if there is cholangiographic evidence of extrahepatic biliary obstruction, beading, and irregularities at least greater than 90 days after transplantation; or if there is histologic evidence of fibrous cholangitis and/or fibro-obliterative lesions with or without ductopenia, biliary fibrosis, or biliary cirrhosis.
Only gold members can continue reading. Log In or Register to continue