Part 2 The upper limb
Development of the musculoskeletal system
Mesodermal somites
By the end of the third week after fertilization the paraxial mesoderm begins to divide into mesodermal somites which are easily recognizable during the fourth and fifth weeks (Fig. 2.1A). Eventually some 44 pairs of somites develop, although not all are present at the same time; however, the paraxial mesoderm at the cranial end of the embryo remains unsegmented. There are 4 occipital somites, followed by 8 cervical, 12 thoracic, 5 lumbar, 5 sacral and 8–10 coccygeal somites. The growth and migration of these somitic cells are responsible for the thickening of the body wall, as well as the development of bone and muscle. The deeper layers of the skin are also of somitic origin. Somite-derived tissue spreads medially to form the vertebrae, dorsally to form the musculature of the back, and ventrally into the body wall to form the ribs, and the intercostal and abdominal muscles.
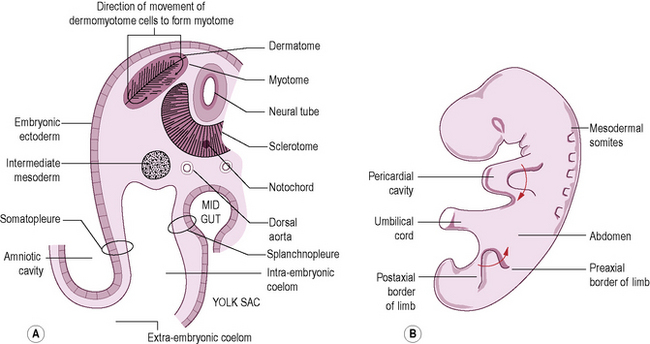
Soon after its formation each somite becomes differentiated into three parts. The ventromedial part forms the sclerotome, which migrates medially towards the notochord and neural tube to take part in the formation of the vertebrae and ribs (Fig. 2.1A). The remainder of the somite is known as the dermomyotome. The cells of the dorsal and ventral edges proliferate and move medially to form the myotome, whose cells migrate widely and become differentiated into myoblasts (primitive muscle cells). The remaining thin layer of cells forms the dermatome, which spreads out to form the dermis of the skin.
Development of the limbs
The limbs initially appear as flipper-like projections (the limb buds), with the forelimbs appearing first, between 24 and 26 days, each bud consisting of a mass of mesenchyme covered by ectoderm with a thickened ectodermal ridge at the tip; the ectodermal ridge controls normal development of the limb. Consequently, damage to it will result in some trauma to the limb. At the beginning of the second month the elbow and knee prominences project laterally and backwards. At about the same time, the hand and foot plates appear as flattened expansions at the end of the limb bud. Between 36 and 38 days, five radiating thickenings forming the fingers and toes can be distinguished, the webs between the thickenings disappear freeing the digits. Appropriate spinal nerves grow into the limbs in association with migration of the myotomes: C5, 6, 7, 8 and T1 for the upper limb, and L4, 5, S1, 2 and 3 for the lower limb. The limb bones differentiate from the mesenchyme of the bud. The limbs grow in such a way that they rotate in opposite directions, the upper limb laterally and lower limb medially (Fig. 2.1B). Consequently, the thumb becomes the lateral digit of the hand, while the great toe is the medial digit of the foot.
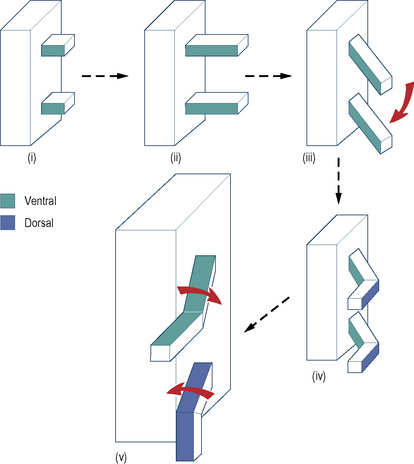
During development the upper limb bud appears as a swelling from the body wall (Fig. 2.2(i)) at the level of the lower cervical and first thoracic segments. At first the limb buds project at right angles to the surface of the body, having ventral and dorsal surfaces and cephalic (preaxial) and caudal (postaxial) borders (Fig. 2.2(ii)). As the limb increases in length it becomes differentiated, during which time it is folded ventrally so that the ventral surface becomes medial (Fig. 2.2(iii)), with the convexity of the elbow directed laterally (Fig. 2.2(iv)). At a later stage the upper and lower limbs rotate in opposite directions so that the convexity of the elbow is directed towards the caudal end of the body (Fig. 2.2(v)). As the limb bud develops, the primitive muscle mass becomes compartmentalized, foreshadowing the adult pattern. Intermuscular septa, extending outwards from the periosteum of the humerus, divide the arm into anterior and posterior compartments. As in the lower limb, some of the anterior compartment musculature has become separated into an adductor group. However, in the upper limb this muscle mass has degenerated phylogenetically so that all that remains is coracobrachialis. Adduction of the upper limb is a powerful action in humans, being served by great sheets of muscle that have migrated into it; these are latissimus dorsi posteriorly and pectoralis major anteriorly. In the forearm, the radius (preaxial bone) and the ulna (postaxial bone) are connected by an interosseous membrane, and to the investing fascia by intermuscular septa. The compartments so formed enclose muscles of similar or related functions.
The upper limit of the upper limb is not so easily defined as in the lower limb. In spite of muscular attachments to the head, neck and thorax, the upper limits can be conveniently considered as the superior surface of the clavicle anteriorly and the superior border of the scapula posteriorly. The free upper limb is divided into the arm between the shoulder and elbow, the forearm between the elbow and the wrist, and the hand beyond the wrist. The hand has an anterior or palmar surface, and a posterior or dorsal surface (Fig. 2.3).
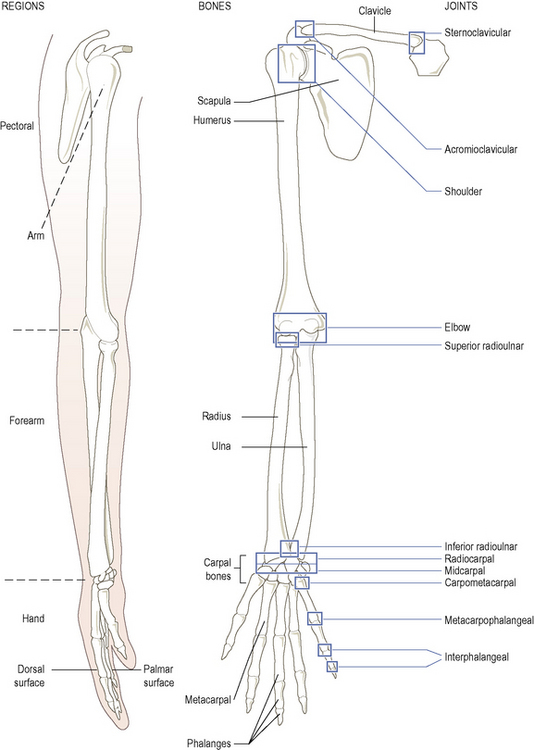
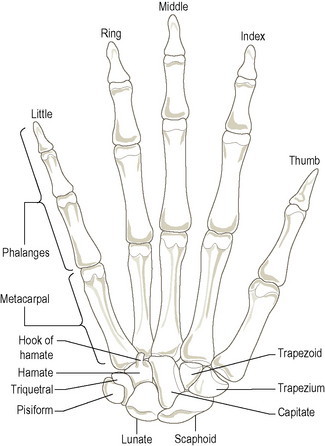
The bones of the upper limb are the clavicle and scapula of the pectoral girdle, the humerus in the arm, the lateral radius and medial ulna in the forearm, the eight carpal bones of the wrist, the five metacarpals of the hand and the phalanges of the digits – two in the thumb and three in each finger (Fig. 2.3).
Bones
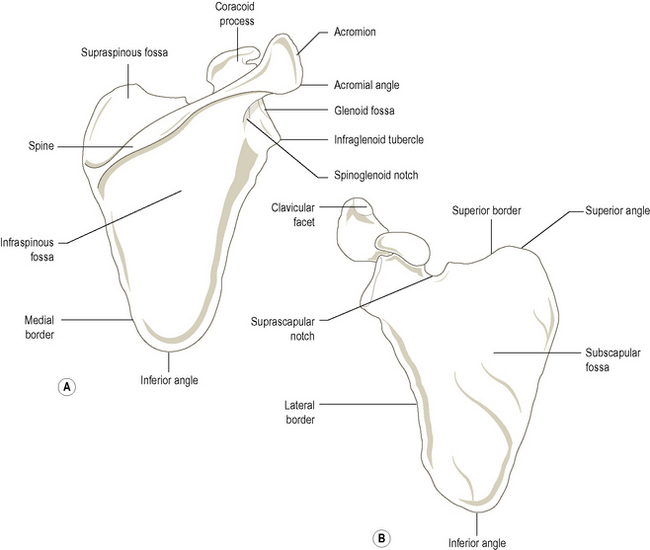
The scapula
This is a large, flat, triangular plate of bone on the posterolateral aspect of the thorax, overlying the second to the seventh ribs. Suspended in muscles, the scapula is held in position by the strut-like clavicle, but retains great mobility relative to the thorax. Being a triangular bone it has three angles, three borders and two surfaces which support three bony processes (Figs. 2.4 and 2.5A).
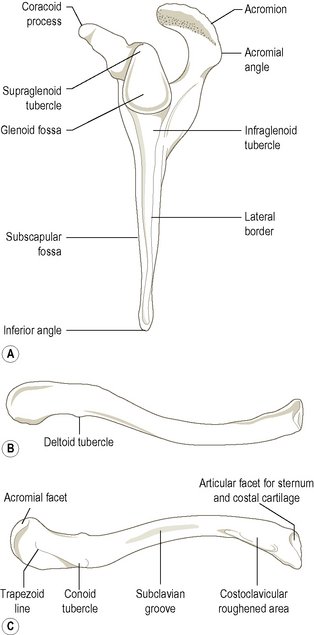
The clavicle
This is a subcutaneous bone running horizontally from the sternum to the acromion (Fig. 2.5B,C). It acts as a strut holding the scapula laterally, thus enabling the arm to be clear of the trunk – an essential feature in primates. The scapula and clavicle together form the pectoral (shoulder) girdle, transmitting the weight of the upper limb to the axial skeleton and facilitating a wide range of movement of the upper limb.
The lateral (acromial) end of the clavicle is the most flattened part and has a small deltoid tubercle on its anterior border. Inferiorly the rounded conoid tubercle is present at the posterior edge, with the rough trapezoid line (Fig. 2.5C) running forwards and laterally away from it. The conoid tubercle and trapezoid line give attachment to the conoid and trapezoid parts of the coracoclavicular ligament binding the clavicle and scapula together. Laterally is a small oval facet for the acromion: it faces obliquely downwards and laterally.
Ossification
Bones of the pectoral girdle
Scapula
The humerus
Largest bone in the upper limb (Fig. 2.6), being a typical long bone with a shaft (body) and two extremities (ends). Proximally, it articulates with the glenoid fossa of the scapula forming the shoulder joint, and distally with the radius and ulna forming the elbow joint.
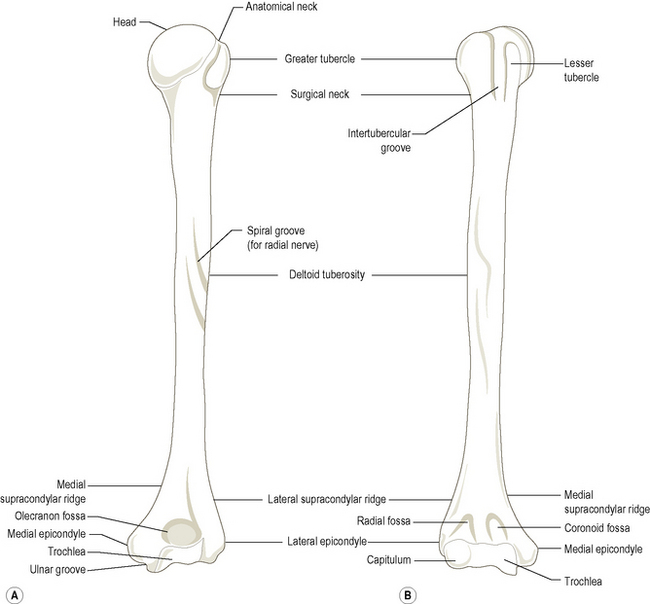
Medial to the capitulum is the trochlea, the articular surface for the ulna. The trochlea is a grooved surface rather like a pulley, the medial edge projecting further distally and anteriorly than the lateral. This causes the ulna also to project laterally and results in a carrying angle between the humerus and ulna (see Fig. 2.79B).
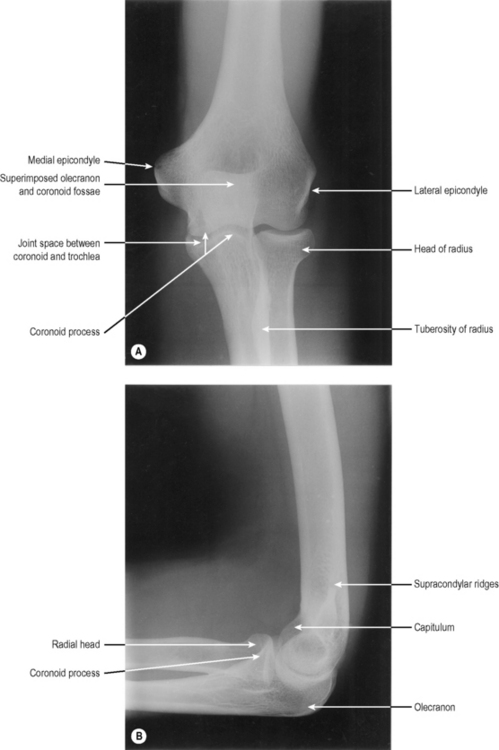
Just above the articular surfaces, the lower end of the humerus presents three fossae for the bony processes of the radius and ulna. Posteriorly is the deep olecranon fossa, which on full extension of the elbow receives the olecranon process of the ulna. Anteriorly, there are two fossae, the lateral radial and medial coronoid fossae, which on full flexion of the elbow receive the head of the radius and coronoid process of the ulna respectively. Many of the bony features previously described can be seen in Figs. 2.7 and 2.9.
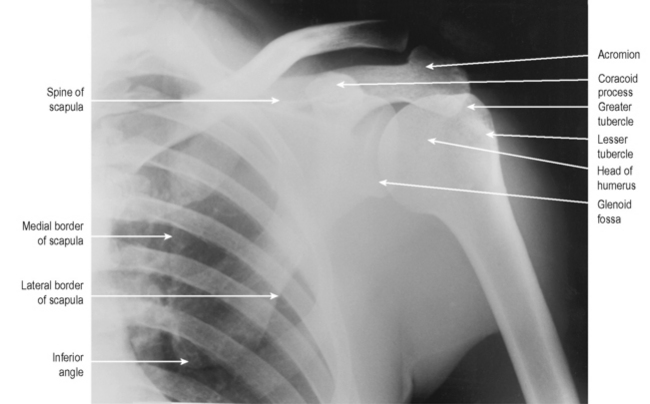
Palpation
At the upper end of the humerus the most lateral bony point at the shoulder is the greater tubercle, whose quadrilateral superior, anterior and posterior surfaces can be felt. Further differentiation can be made by palpating the lateral margin of the acromion (p. 41) and then running the fingers off its edge onto the greater tubercle. The rounded lesser tubercle can be felt through the deltoid, and is just lateral to the tip of the coracoid process. To the lateral side of the lesser tubercle the impression of the intertubercular sulcus can usually be felt. The shaft of the humerus is covered with thick muscle, but can be palpated on its medial and lateral sides. At the lower end, the prominent medial epicondyle is the most obvious bony landmark. The ulnar nerve can be rolled in the groove behind it (the ‘funny bone’). Running upwards from the medial epicondyle the sharp medial supracondylar ridge can be palpated. The lateral epicondyle can be palpated at the base of a dimple on the lateral aspect of the elbow, as can the lateral supracondylar ridge running upwards from it. Posteriorly, the olecranon fossa can be felt through the triceps tendon, if the relaxed elbow is flexed.
Ossification
The bones of the forearm are the radius laterally and the ulna medially, which articulate proximally with the humerus at the elbow joint and contribute to the wrist joint distally. They are connected by a strong interosseous membrane between their shafts, and synovial pivot joints at each end. Both are long bones, the ulna being expanded proximally and the radius distally (Fig. 2.8A,B). The shaft of the radius is convex laterally, allowing it to move around the ulna carrying the hand with it in pronation of the forearm.
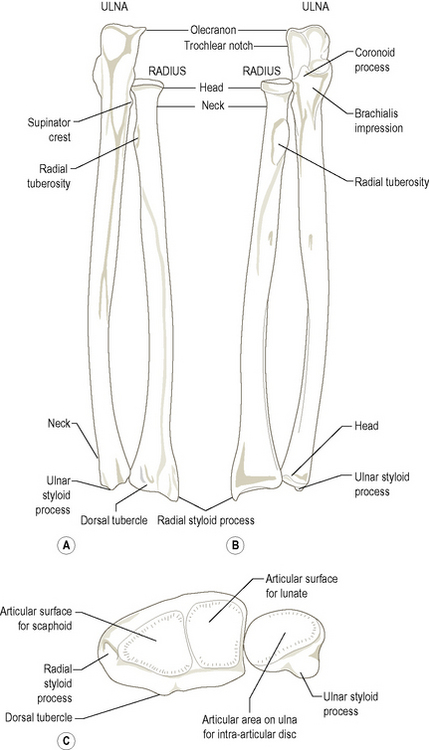
The radius
The inferior end of the radius is expanded having five distinct surfaces. The lateral surface, which extends down to the styloid process, has a shallow groove anteriorly for the tendons of the abductor pollicis longus and extensor pollicis brevis. The medial surface forms the concave ulnar notch for articulation with the head of the ulna: it has a roughened triangular area superiorly. The posterior surface is convex and grooved by tendons. The prominent ridge in the middle of this surface is the dorsal (Lister’s) tubercle. The lateral half of this surface continues down onto the styloid process. The anterior surface is smooth and curves forward to a distinct anterior margin. The distal articular surface is concave and extends onto the styloid process; it is divided by a ridge into two areas, a lateral triangular area for articulation with the scaphoid and a medial quadrilateral area for the lunate (Fig. 2.8C).
The ulna
The ulna lies medial to the radius and is the longer of the two bones. It has a shaft and two ends, of which the superior is the larger presenting as a hook-like projection for articulation with the trochlea of the humerus. The smaller rounded distal end is the head of the ulna (Fig. 2.8B): it does not articulate directly with the carpus. The ulna articulates laterally at each end with the radius.
The coronoid process projects from the front of the shaft and has an upper articular surface which completes the trochlear notch (Figs. 2.8B and 2.9). These two surfaces are often separated by a roughened non-articular area running horizontally across the notch. The trochlear notch is divided by a vertical ridge into a larger medial part and a smaller lateral part, the latter being continuous over its outer edge with the articular surface of the radial notch on the lateral side of the coronoid process. There is a small tubercle where the medial and anterior edges of the articular surface of the coronoid process meet; this gives attachment to the anterior part of the ulnar collateral ligament. The irregular, anterior surface of the coronoid ends inferiorly as the rough tuberosity of the ulna. Both this surface and the tuberosity give attachment to brachialis. At the upper medial part of the coronoid is the small sublime tubercle from which the pronator ridge runs downwards and laterally.
Ossification
Bones of the arm and forearm
Humerus
Radius