Part 4 The trunk and neck
Introduction
One of the major features distinguishing human beings from other animals is their bipedal posture and gait. As the hindlimbs progressively took over the locomotor function, the vertebral column assumed a new role. No longer is it held horizontally (Fig. 4.1A), where it is under compression, but it has become a vertical weight-bearing rod, held erect by ligaments and muscles (Fig. 4.1B). This change in function of the vertebral column has been accompanied by changes in its form, as well as by changes in its relationship to the skull and pelvic girdle.
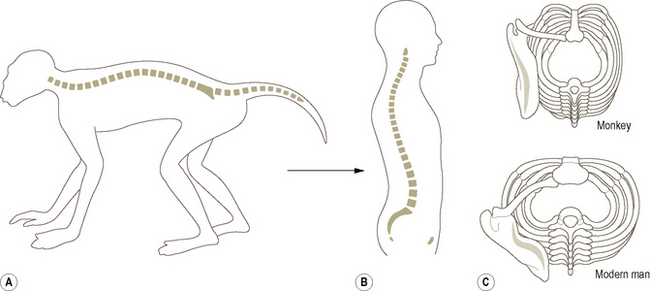
First, the vertebral bodies increase in size towards the lumbar region (Fig. 4.1B) because the compression forces along the trunk are no longer constant but increase progressively from above downwards. The proportions of the vertebral bodies also change from above downwards. Second, the spinous processes are more or less equally developed along the length of the vertebral column because the tendency to bend is no longer restricted to the limb girdles (the points of support), but is more evenly distributed. This is perhaps most clearly seen in the cervical region because the human head is more or less balanced on the vertebral column. Thirdly, the stiffening effect of the sternum and abdominal muscles on the vertebral column has become less important. The sternum has come to lie nearer the vertebral column so that the thorax is wider and less deep (Fig. 4.1C). This has resulted in a less abrupt change in direction of the ribs at their angles. Finally, the increased weight transmission through the pelvis and legs has brought about an enlargement of the sacrum, so that the human sacrum is usually composed of five fused segments. It is also relatively wide and more convex on its pelvic surface.
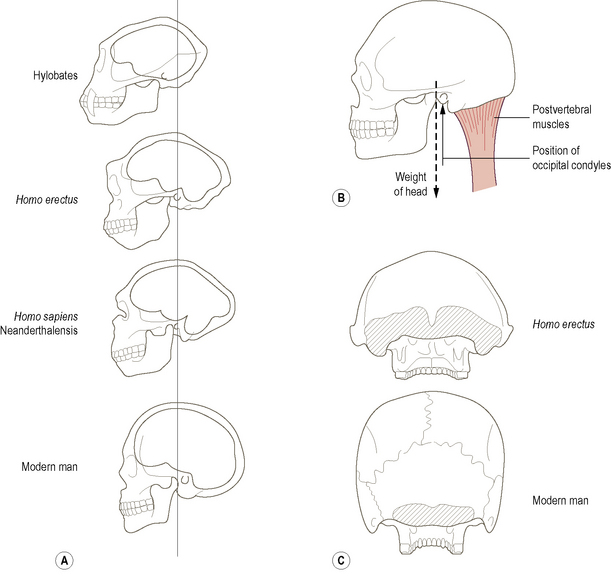
Concomitant with the changes in the vertebral column and trunk, the relation and form of the skull and its associated musculature have also changed dramatically. In quadrupedal animals, the head is supported by the postvertebral (nuchal) muscles and ligaments (these being under tension), which produce compression of the cervical vertebrae. As a more erect posture evolved the strength required in the postvertebral muscles was reduced because more of the weight of the head was carried directly by the vertebrae. This was accompanied by a reduction in the muzzle and an enlargement of the brain (Fig. 4.2A) causing the centre of gravity of the head to move more nearly over the point of support (the occipital condyles). It would be undesirable to have the head perfectly balanced on the occipital condyles because humans possess no powerful prevertebral muscles to support the skull from the front. Consequently, the centre of gravity projection falls just anterior to the occipital condyles, being balanced by the postvertebral muscles (Fig. 4.2B). That the postvertebral muscles have been reduced in importance is evident from the relatively small area of their attachment to the skull in humans compared with other primates (Fig. 4.2C).
The vertebral column comprises a series of mobile segments held together by ligaments and muscles, each separated from adjacent segments by an intervertebral disc. There are usually 33 bony segments, of which only 24 present as separate bones: the lower nine are fused, five forming the sacrum and four the coccyx. The 24 presacral vertebrae are designated cervical, thoracic and lumbar according to their features and position within the trunk: there are seven cervical, twelve thoracic and five lumbar vertebrae (Fig. 4.3). The length of the vertebral column is between 72 and 75 cm for the majority of individuals, of which approximately one-quarter is accounted for by the intervertebral discs. About 40% of an individual’s height is due to the length of the vertebral column. Variations in height between individuals mainly reflect differences in lower limb length rather than differences in vertebral column length. However, diurnal variations in height, up to 2 cm between early morning and late evening, are due to compression and loss of thickness of the individual intervertebral discs. (It is as well to remember this when charting the change in height of an individual.) Loss of height in elderly individuals is associated with thinning of the discs as a result of age-related changes within them.
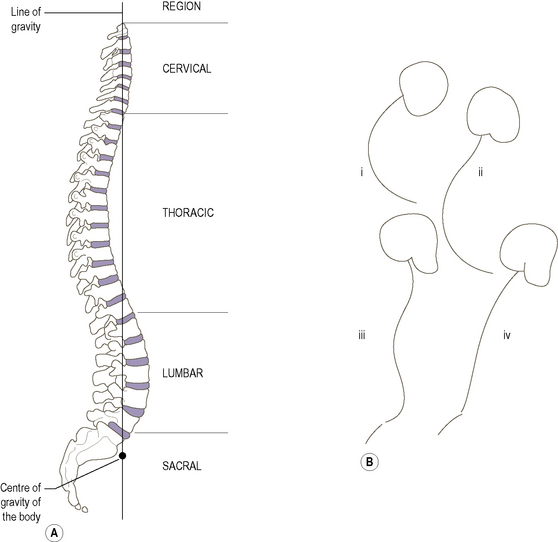
The adult vertebral column has four curvatures (Fig. 4.3A), an anterior convexity in the cervical and lumbar regions, and an anterior concavity in the thoracic and sacrococcygeal regions. Both the cervical and lumbar curvatures are acquired, in the sense that they are not present in early fetal development. Until late in fetal development, the vertebral column shows a single curvature concave anteriorly (Fig. 4.3B(i)). Late in fetal life the secondary cervical curvature (Fig. 4.3B(ii)) begins to appear, becoming more accentuated between 6 and 12 weeks after birth as the infant begins to hold up its head to enlarge its visual environment. The secondary lumbar curvature (Fig. 4.3B(iii)) appears when the child begins to sit up at around 6 months, becoming more marked with standing and the onset of walking. It is the extension of the hip that accompanies standing and walking which tilts the pelvis forwards so that the axis of the pelvic cavity is no longer in line with that of the abdominal cavity. The lumbar curvature develops in order to keep the trunk erect when standing. The lumbar curvature is not fully developed until after the age of 2, when a more or less adult pattern of walking is established. Sadly, in old age the vertebral column tends to assume a gentle C-shaped curve (Fig. 4.3B(iv)) reminiscent of the early fetal curve. The reason being that the shape of the vertebral column is largely determined by the intervertebral discs, and to a much lesser extent by the vertebrae themselves. Consequently, as the discs degenerate and thin with increasing age the secondary curvatures gradually disappear.
The vertebral curves pass in front of and behind the line of gravity along which the weight of the head, upper limbs and trunk is projected to the lower limbs. This line is said to pass progressively through the dens, the bodies of the second and 12th thoracic vertebrae and the promontory of the sacrum (Fig. 4.3), with the centre of gravity of the body located just in front of the sacral promontory. However, it must be remembered that the line of gravity is not constant; it is continually changing, both as the body moves and also when standing still. Nevertheless, it is a useful concept in reminding us of the natural balance and beauty of the body. By visualizing changes in the projection of this line, it may be possible to determine the structures put under increased strain in certain postures and pathologies.
Embryological development of the vertebrae
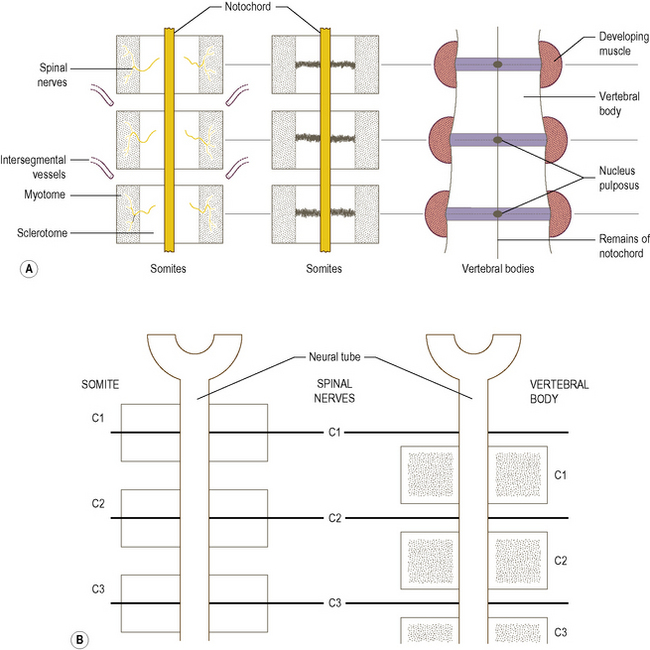
Soon after the formation of each somite it becomes differentiated into the three parts, the ventromedial sclerotome, the medial myotome and the thin lateral dermatome. The sclerotomes come to surround the notochord, followed by the myotomes. Each vertebra is formed from the adjacent parts of two sclerotomes (Fig. 4.4), with the intervening part forming the outer part (annulus fibrosus) of the intervertebral disc. The nucleus pulposus of the disc is derived from the notochord. As there are eight cervical somites, there are also eight cervical nerves, similarly in the thoracic, lumbar and sacral regions. However, because each vertebra is formed from adjacent somites the cervical nerves come to lie above their correspondingly numbered vertebrae, with the eighth cervical nerve lying below the seventh cervical vertebra. The thoracic, lumbar and sacral spinal nerves all lie below their correspondingly numbered vertebrae.
The vertebral column
With the exception of the first and second cervical vertebrae, all vertebrae possess a large weight-bearing body anteriorly and vertebral arch posteriorly, which consists of a series of bony processes (Fig. 4.5A). The body varies in shape and size depending on its location in the vertebral column, but is roughly cylindrical with flattened upper and lower surfaces. On these surfaces, the markings of the attachment of the intervertebral disc around the periphery can be seen surrounding a roughened central area. The front and sides of the bodies are roughened, particularly at their upper and lower edges, and concave from top to bottom. The posterior surface is fairly smooth and has a large foramen for the passage of the basivertebral vein. The vertebral arch arises from the posterolateral aspect of the body, and with the body surrounds the vertebral foramen. In situ adjacent vertebral foramina, together with the intervertebral discs and the ligamenta flava, form the vertebral canal which houses the spinal cord and its various coverings.
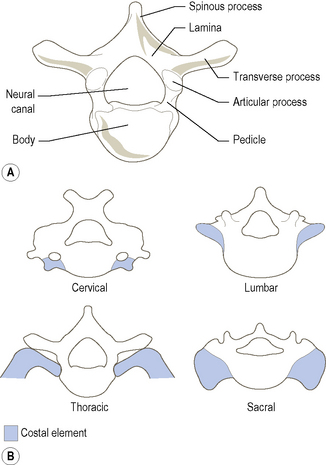
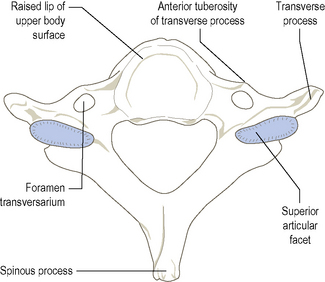
With a few exceptions, each part of a vertebra is potentially present in every other vertebra, the main features of which are shown in Fig. 4.5A. The body is the only part of a vertebra that is represented throughout the whole series of vertebrae; even so, that of the atlas has been displaced as the dens of the axis. The major difference between cervical, thoracic, lumbar and sacral vertebrae is related to the size and fate of their costal elements (Fig. 4.5B). In the cervical region, the medial end of the costal element fuses with the side of the vertebral body. The presence of the vertebral vessels lying anterior to the true transverse process prevents complete fusion of the costal element with the transverse process. Instead, a costotransverse lamella (bar) joins the two parts together laterally, leading to the formation of the foramen transversarium. Consequently, the anterior tubercle of the transverse process is the lateral end of the costal element, while the posterior tubercle represents the lateral end of the transverse process. The first and second cervical vertebrae have no anterior tubercles.
Bones
A description of the sacral and coccygeal vertebrae can be found on pages 211–213.
Lumbar vertebrae
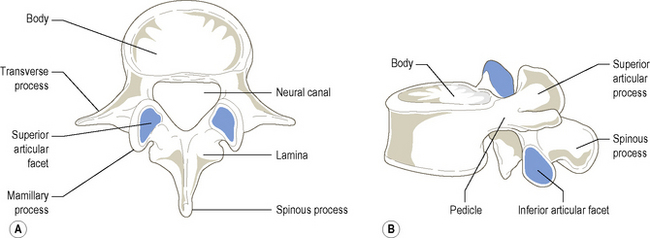
The five lumbar vertebrae are much stouter and stronger than those in either the thoracic or cervical regions (Fig. 4.6). They possess neither foramina transversaria nor articular facets for the ribs. Each has a large, kidney-shaped body with almost parallel upper and lower surfaces, except for L5 which is deeper anteriorly than posteriorly. The short strong pedicles pass almost directly backwards to join the narrow laminae which pass backwards and medially towards the spine. Adjacent laminae are widely separated from each other, leaving diamond-shaped spaces which contain the ligamenta flava.
Thoracic vertebrae
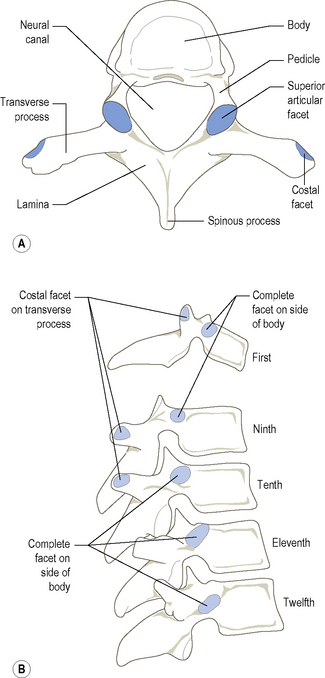
The distinctive feature of thoracic vertebrae is the presence of articular (costal) facets on the sides of the vertebral body for articulation with the heads of at least one pair of ribs (Fig. 4.7). The bodies of thoracic vertebrae are typically heart-shaped, when viewed from above, and on their sides bear articular facets. The bodies of the second to eighth vertebrae have large, almost complete oval facets near their upper borders, and smaller demifacets near their lower borders. Although similar in basic arrangement, the upper facet of the ninth thoracic vertebra is situated at the base of the pedicle. The body of T1 has a complete oval facet near its upper edge and a demifacet at its lower. The 10th, 11th and 12th vertebrae have single complete facets located at the junction of the body with the pedicle. Between T10 and T12 the facets gradually move from the upper to lower region of the junction (Fig. 4.7B).
From just medial to the base of the transverse process, the articular processes project almost vertically, the superior upwards and the inferior downwards. The articular facets on the superior process are slightly concave transversely, being flat from above down, and face backwards but also slightly upwards and laterally. The facets on the shorter inferior articular processes are reciprocally curved and face in the opposite direction. The superior articular facets of one vertebra articulate with the inferior facets of the vertebra above. The joints so formed lie on the arc of a circle whose centre lies within or just anterior to the body of the vertebra. Consequently, rotation as well as flexion and extension are favoured in the thoracic region (p. 463).
Cervical vertebrae
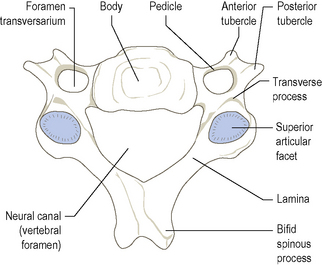
The characteristic feature of all cervical vertebrae is the presence of a foramen transversarium in each transverse process (Fig. 4.8). They tend to be small as they do not carry much weight. The third, fourth, fifth and sixth cervical vertebrae are sufficiently similar to be considered together. The body is relatively small, appearing kidney-shaped when viewed from above. Its superior surface projects upwards at the sides, while its inferior surface is correspondingly bevelled. Between the sides of adjacent surfaces of the bodies, each side of the intervertebral disc, are small synovial joints (uncovertebral joints, p. 451). The anterior surface is marked by the attachment of the anterior longitudinal ligament, while laterally the body is hollowed. The posterior surface of the body is flat.
The seventh cervical vertebra
The seventh vertebra (Fig. 4.9), also known as the vertebra prominens, is noted for the length of its non-bifid spinous process. It is larger than the preceding cervical vertebra and exhibits similarities to thoracic vertebrae. The body is larger, the pedicles are directed more posteriorly than laterally, the inferior articular facets face more anteriorly than downwards, and the vertebral canal is generally smaller than that of other cervical vertebrae.
The axis (C2)
The axis (C2), the second and strongest of the cervical vertebrae, has many of the features of a typical cervical vertebra (Fig. 4.10). It has, however, the separated body of the atlas fused with the superior surface of its body giving an upward tooth-like projection known as the odontoid process (dens). The dens is slightly pointed at its apex, where the apical ligament attaches it to the anterior margin of the foramen magnum. From the sloping sides of the apex, alar ligaments pass to tubercles on the medial sides of the occipital condyles. Its anterior surface has a small smooth facet, concave from above down and convex transversely for articulation with the facet on the back of the anterior arch of the atlas. Posteriorly is a smooth, constricted horizontal surface where the transverse ligament crosses. Above this constriction there is a slightly expanded area known as the head.
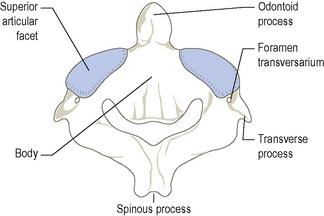
The inferior surface of the axis is very similar to that of a typical cervical vertebra (Fig. 4.8).
The atlas (C1)
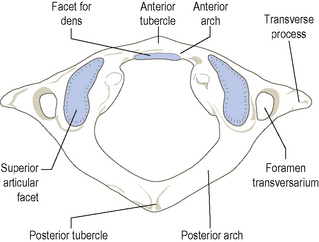
This ring of bone bears very little resemblance to a cervical or for that matter any other vertebra (Fig. 4.11). It has no body or spine, but consists of slender anterior and posterior arches joined on each side by a lateral mass, which bears articular facets superiorly and inferiorly and a transverse process laterally. The concave superior facets articulate with the condylar processes of the occipital bone, while the concave inferior facets articulate with the second cervical vertebra. The inferior articular facets are segments of a sphere, thereby facilitating rotation between the atlas and axis. Each lateral mass is marked on its medial side by a small tubercle to which the transverse ligament of the atlas attaches.
The vertebrae
Typical thoracic vertebra
Typical cervical vertebra
The vertebral column
Ossification of the vertebrae
Many congenital conditions of the vertebral column are due to incomplete fusion of its constituent parts. Hemivertebrae can cause an abnormal lateral curvature (scoliosis) of the vertebral column. The laminae may fail to fuse or meet in any region, but most commonly in the lumbosacral region, giving rise to spina bifida. The spine, laminae and inferior articular processes of L4 and L5 may be joined to the rest of the vertebrae by cartilage and not completely fused. Under certain loading conditions this can lead to a separation whereby the vertebral body, most commonly that of L5, slides forwards. This condition is known as spondylolisthesis (see p. 284).



