• Solitary, slowly growing, and often long-standing lesion
• Treatment: Complete excision
• Excellent prognosis
• Low rate of recurrence, usually related to incomplete excision
Macroscopic
• Usually < 5 cm (median: 1.5 cm)
Microscopic
• Moderately cellular proliferation of spindled to stellate fibroblastic cells in randomly arranged loose fascicles or storiform arrays
• Nuclear atypia minimal to absent
• Rare mitoses; no necrosis
• Variable myxoid, myxocollagenous, or collagenous stroma
• Mast cells common
Ancillary Tests
• CD34(+)
• Negative for S100, desmin, keratin, claudin-1
Top Differential Diagnoses
• Dermatofibroma (fibrous histiocytoma)
• Perineurioma
• Acquired digital fibrokeratoma
• Dermatofibrosarcoma protuberans
• Myxoid neurofibroma
SAF Superficial acral fibromyxoma (SAF), also referred to as digital fibromyxoma, is a benign fibroblastic tumor that shows a marked predilection for the fingers and toes, particularly the nail bed region. Histologically, it is characterized by bland spindled and stellate cells arranged in random loose fascicles and storiform arrays within a variable myxoid to fibrous stroma.
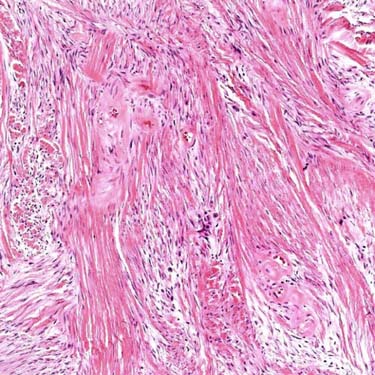
Prominent Collagen in SAF Some areas of SAF feature prominent stromal collagen, as depicted.
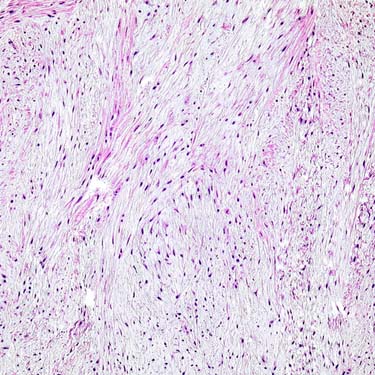
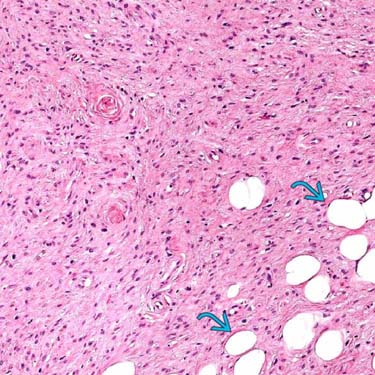
Loose Storiform Growth in SAF SAF may also demonstrate a loose arrangement of cells in a more vascularized stroma, somewhat resembling perineurioma. Despite its usual dermal origin, in some cases, SAF shows superficial extension into subcutaneous fat .
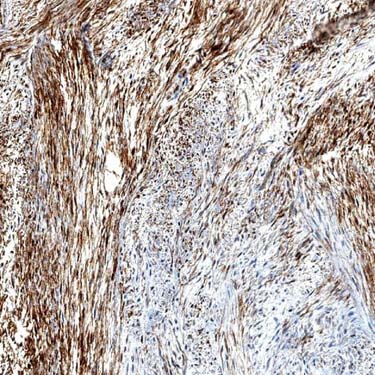
CD34 Expression in SAF CD34 expression is seen in most cases of SAF, but the extent of this positivity varies. Focal EMA and SMA may also be seen in rare cases. S100, claudin-1, desmin, and keratins are negative.
TERMINOLOGY
Abbreviations
• Superficial acral fibromyxoma (SAF)
Synonyms
• Acral fibromyxoma
• Digital fibromyxoma
• Cellular digital fibroma
Definitions
• Benign fibroblastic neoplasm that occurs in hands and feet, particularly nail bed region
CLINICAL ISSUES
Epidemiology
• Incidence
Rare
• Age
Wide age range
– Most common > 40 yr
• Sex
Male predilection
Site
• Almost exclusively on hands and feet
Vast majority in fingers and toes
– Particularly subungual or periungual region (nail bed)
• Extremely rare in nonacral sites
Presentation
• Solitary, slowly growing, and often longstanding lesion
Associated with pain in up to 40-50% of cases
• Superficial, dermal based
Treatment
• Complete excision
Prognosis
• Excellent prognosis
• Recurrences have been reported in up to 22%
Only gold members can continue reading. Log In or Register to continue
 .
.