Squamous Hyperplasia
Antonio L. Cubilla, MD
Alcides Chaux, MD
Elsa F. Velazquez, MD
Key Facts
Terminology
Thickening of mucosal squamous epithelium without atypia
Most common epithelial alteration associated with penile cancer
Frequently associated with differentiated PeIN
Found in association with usual, papillary, and verrucous SCC (HPV-unrelated variants of SCC)
Macroscopic Features
Whitish areas with irregular borders
Microscopic Pathology
Acanthosis with hyperkeratosis
Normal maturation with no atypias
Parakeratosis is uncommon
Koilocytes are absent
Merging of SH with PeIN &/or invasive SCC is common finding
Flat squamous hyperplasia is most common pattern
Other subtypes include papillary, pseudoepitheliomatous, and verrucous
Mixed forms represent about 1/3 of cases
Top Differential Diagnoses
Differentiated PeIN
Warty PeIN
Basaloid PeIN
Warty/basaloid PeIN
Pseudohyperplastic SCC
Verruciform xanthoma
Warty, papillary, and verrucous carcinomas
 Squamous hyperplasia typically presents as whitish pearly areas  with irregular borders merging with an adjacent in situ or invasive component with irregular borders merging with an adjacent in situ or invasive component  . . |
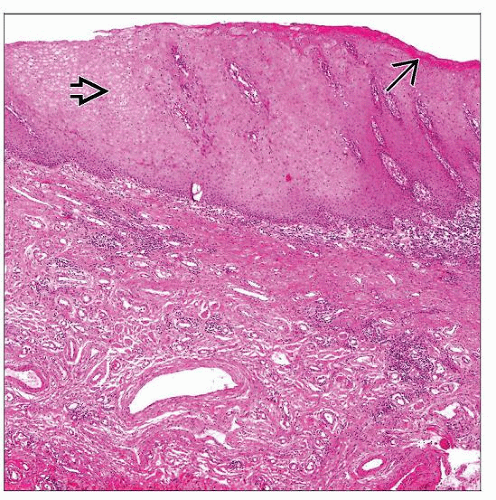 Squamous hyperplasia is characterized by acanthosis  , retained epithelial maturation, absence of cytologic atypia, hyperkeratosis , retained epithelial maturation, absence of cytologic atypia, hyperkeratosis  , and a flat surface. , and a flat surface. |
TERMINOLOGY
Abbreviations
Squamous hyperplasia (SH), squamous cell carcinoma (SCC), penile intraepithelial neoplasia (PeIN)
Definitions
Thickening of mucosal squamous epithelium without cytologic atypia
ETIOLOGY/PATHOGENESIS
Pathogenesis
Unknown
Reactive condition rather than specific entity
Most common epithelial change associated with penile cancer
Almost all keratinizing SCC have associated SH
May be associated with reactive inflammatory conditions
CLINICAL ISSUES
Site
SH may affect any penile mucosal compartment
Presentation
Usually found in continuity or slightly distant from in situ or invasive SCC
Distinction between SH and normal mucosa may be subtle
Inapparent lesions may be better visualized with acetic acid (peniscopy)
Clinically, it may be difficult to distinguish from PeIN
Micaceous balanitis and penile horn are clinically florid forms of SH with prominent hyperkeratosis
Treatment
Benign epithelial change and usually no treatment is required
Prognosis
May be precursor lesion of HPV-unrelated variants of SCC, but more studies are required to confirm this hypothesis
MACROSCOPIC FEATURES
General Features
Whitish areas with irregular borders
Slightly raised areas with pearly appearance
MICROSCOPIC PATHOLOGY
Histologic Features
Acanthosis with orthokeratotic hyperkeratosis
Normal epithelial maturation
Chronic inflammation may be present
Absence of cytologic atypia
Absent koilocytosis
Minimal to absent parakeratosis
Absent intraepithelial keratin whorls (pearls)
Associated with lichen sclerosus in some cases
Frequently associated with differentiated PeIN
Usually found in association with usual, papillary, and verrucous SCC (HPV-unrelated variants of SCC)
Rarely present adjacent to condylomatous (warty) and basaloid SCC
Merging of SH with PeIN &/or invasive SCC is common finding
Histological Subtypes
Flat
Most common subtype
Nonatypical acanthosis
Hyperkeratosis with orthokeratosis
Linear interface between basal layer and stroma
Papillary
Represents minority of cases
Serrated appearance on low-power view
Jagged interface with underlying stroma
Nonatypical acanthosis with short hyperkeratotic papillae
Pseudoepitheliomatous
Unusual pattern of SH
Acanthosis
Downward elongated proliferation of rete ridges that appear detached from epithelium
Regular epithelial nests with peripheral palisading
Stromal reaction is not prominent
Typically associated with papillary SH
Verrucous
Present adjacent to verrucous carcinoma
Marked acanthosis with no atypia
Hyperkeratosis with hypergranulosis
Slight papillomatosis
Mixed
2nd most common type
Presence of mixed areas of flat and papillary SH
DIFFERENTIAL DIAGNOSIS
Differentiated PeIN
Acanthosis, parakeratosis
Aberrant keratinization with cytologic atypia
Retained squamous maturation
Warty/Basaloid PeIN
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


