Other Tumors and Tumor-like Lesions of the Renal Pelvis
Satish K. Tickoo, MD
Victor E. Reuter, MD
Key Facts
Terminology
Neoplasms other than usual urothelial carcinoma involving upper urinary tract
Clinical Issues
Most carcinomas with nontransitional cell features in pelvis exist in association with usual urothelial (transitional cell) carcinomas
Pure nonurothelial carcinomas of pelvis are very rare
Microscopic Pathology
Inverted papilloma with endophytic interconnected trabeculae and cords of urothelium, extensively invaginating from surface into lamina propria
Nephrogenic metaplasia/adenoma shows multiple architectural patterns, including papillary, tubular/glandular, cystic, single cells, and sheet-like
Typically, thick basement membrane/hyalinized sheath surrounds epithelium
Squamous cell carcinoma usually accompanied by extensive squamous metaplasia of urothelium and squamous cell carcinoma in situ
Adenocarcinoma shows various phenotypes, including glandular NOS, enteric, micropapillary, signet ring/plasmacytoid, mucinous
Benign nonepithelial tumors include fibroepithelial polyp, inflammatory myofibroblastic tumor, hemangioma, angiomyolipoma, leiomyoma, neurofibroma
Top Differential Diagnoses
Metastatic tumors
Urothelial carcinoma with inverted growth pattern
 All aberrant morphologies of urothelial carcinoma seen in the bladder may be seen in the upper tract. Adenocarcinomas may be pure but often appear in association with a urothelial component  . . |
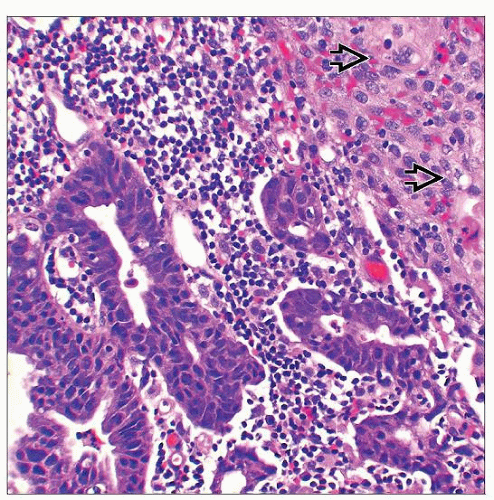
 Squamous cell carcinoma, seen here invading the renal parenchyma  , is the 2nd most common carcinoma in the pelvis. Most cases occur as aberrant differentiation in UC, but pure forms may be seen. , is the 2nd most common carcinoma in the pelvis. Most cases occur as aberrant differentiation in UC, but pure forms may be seen. |
TERMINOLOGY
Definitions
Neoplasms other than usual urothelial carcinoma involving upper urinary tract
ETIOLOGY/PATHOGENESIS
Nephrolithiasis and Repeated Infections
Squamous cell carcinoma and adenocarcinoma often occur in background of nephrolithiasis
Reported incidence of coexisting calculus disease in squamous cell carcinoma of renal pelvis varies from 18-100%
Squamous cell carcinoma is often associated with squamous metaplasia of urothelium
Adenocarcinoma is usually associated with intestinal metaplasia, which is regarded as putative precursor of adenocarcinoma
Bladder Cancer
Most cases of renal pelvic urothelial (transitional cell) carcinoma are associated with prior, concurrent, or subsequent bladder carcinoma
However, for nontransitional cell carcinomas of upper tract, such association is not observed
CLINICAL ISSUES
Epidemiology
Incidence
Most carcinomas with nontransitional cell features in pelvis coexist with usual urothelial (transitional cell) carcinomas of pelvis
Pure nonurothelial carcinomas of renal pelvis are very rare
Squamous cell carcinoma is 2nd most common carcinoma of renal pelvis
Incidence of 10% of renal pelvic cases is reported in older study; likely includes urothelial carcinomas with squamous differentiation
More recent studies report a combined incidence of < 1% for squamous cell carcinomas and adenocarcinomas of renal pelvis
All other types of carcinoma in the literature exist as case reports or small case series
Benign epithelial, mesenchymal, and other tumors are also very rare
Fibroepithelial polyps, although more common in adults, are most common benign polypoid ureteric tumors in children
Age
Carcinomas: Range 41-87 years (mean: 66)
Fibroepithelial polyps: Range 7-73 years (mean: 40)
Inverted papillomas: Range 19-89 years (mean: 64)
Primitive neuroectodermal tumors: Mostly young adults/adolescents; range 10-60 years (mean: 27)
Other tumors: Variable, mostly older adults
Presentation
Flank pain &/or hematuria common presentations
Ureteral or pelvi-ureteric junction obstruction with resultant hydronephrosis also not uncommon
Episodic colicky pain, especially in tumors of ureter
Treatment
Surgical approaches
Usually nephroureterectomy performed for carcinomas of pelvis or proximal-most ureter
Malignant tumors of more distal ureters may be amenable to ureterectomy
Polypoid smaller benign tumors, particularly fibroepithelial polyps, may be resected endoscopically
Prognosis
Most pure nontransitional cell, as well as urothelial carcinomas with divergent/aberrant differentiation, are high-grade and high-stage tumors
Most patients with pT3 or pT4 tumors die of disease, and 5-year survivals are extremely uncommon
Some of benign tumors may cause obstruction and resultant hydronephrosis, with related complications
MACROSCOPIC FEATURES
General Features
Carcinomas
Usually large bulky tumors, filling pelvicalyceal system, usually with renal parenchymal and renal sinus soft tissue invasion
Fibroepithelial polyps, hemangiomas, squamous papillomas, and nephrogenic adenomas
Mostly polypoid lesions in pelvis or ureter
Size usually small (mean: 2 cm; mostly 0.5-4 cm in maximum diameter); rare tumors are much larger
Inverted papillomas
Smooth surfaced and often broad based, sessile and domed, rarely pedunculated
More common in ureter than pelvis
Malignant mesenchymal tumors
Often arising in perirenal and renal hilar soft tissues, and secondarily involving pelvicalyceal system and renal parenchyma
MICROSCOPIC PATHOLOGY
Histologic Features
Benign epithelial tumors/lesions
Inverted papilloma
Endophytic interconnected trabeculae and cords of urothelium, extensively invaginating from surface into lamina propria
Covered by flat-surfaced urothelium
Periphery of cords typically show palisading of basal nuclei
Tumor periphery is smooth and pushing, and no desmoplastic stromal reaction is present
Some cases show small glandular structures lined by metaplastic mucinous epithelium
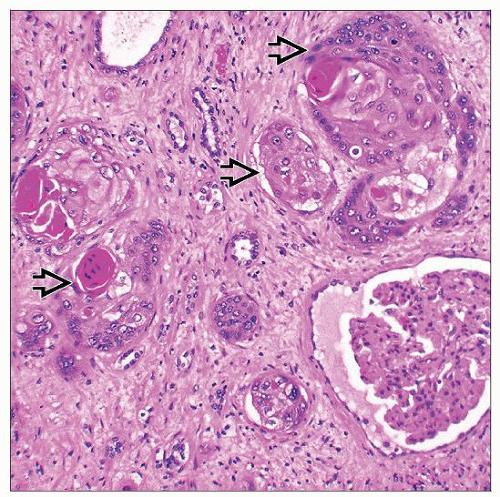
Nephrogenic metaplasia/adenoma
Shows wide spectrum of architectural patterns, with cases often showing mixed patterns
Architectural patterns include papillary, tubular/glandular, cystic, single cells, and sheet-like
Lining epithelial cells are cuboidal and single layered, or occasionally “hobnailed”
Cytoplasm varies from eosinophilic to clear; prominent nucleoli may be present
In single cell areas, cells may show minute lumina, and closely mimic blood vessels or signet ring cells
Typically, thick basement membrane/hyalinized sheath surrounds epithelium
Often associated with inflammatory infiltrate
Villous adenoma
Similar to villous adenomas of colorectum
Biopsy-based diagnosis of villous adenoma should not be made, as adenocarcinoma in vicinity may be missed
Until thorough evaluation of completely excised resection specimen performed, terminology, such as “biopsy fragments with histology of at least villous adenoma,” may be used
Other rare benign epithelial lesions include squamous and urothelial papillomas
Malignant epithelial tumors
Squamous cell carcinoma
More common in renal pelvis than ureter; often associated with nephrolithiasis
Usually accompanied by extensive squamous metaplasia of urothelium and squamous cell carcinoma in situ
Often high stage, frequently with renal parenchymal invasion
Adenocarcinoma
Variety of morphologic phenotypes seen, similar to that in bladder
Different morphologic forms include glandular NOS, enteric, signet ring, mucinous
Often accompanied by glandular and intestinal metaplasia of surrounding urothelium, or occasionally by villous adenoma
Usually high-stage tumors, often with renal parenchymal invasion
Other rare forms of carcinoma (Ca) include
Small cell and large cell neuroendocrine Ca, lymphoepithelioma-like Ca, sarcomatoid Ca, hepatoid Ca, rhabdoid Ca, and lipid-rich Ca
Benign nonepithelial tumors/lesions
Fibroepithelial polyp
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


