Testicular “Tumor” of Adrenogenital Syndrome
Steven S. Shen, MD, PhD
Jae Y. Ro, MD, PhD
Key Facts
Terminology
Benign bilateral testicular tumor in patients with congenital adrenal hyperplasia leading to growth of adrenal-like cells in testis that resembles Leydig cell tumor
Clinical Issues
Age: Children to early adult (average: 22.5 years)
Presentation
Bilateral orchialgia (92%)
Testicular masses (2/3 palpable)
Exogenous high-dose corticosteroids are standard medical treatment (pain control, regression of tumor)
Macroscopic Features
Well-circumscribed but not encapsulated, dark brown, lobulated mass with fibrous septa
Often bilateral (83%), frequently multiple nodules
Microscopic Pathology
Sheets, nests, cords, nodules, or diffuse proliferation of large cells separated by band of fibrous tissue
Polyhedral or polygonal cells resembling Leydig cells
Abundant eosinophilic cytoplasm with lipofuscin pigment
Centrally located nuclei and prominent nucleoli
Frequent nuclear pleomorphism, but no or rare mitoses
Lack of Reinke crystalloid material
Ancillary Tests
Positive for vimentin, inhibin, Melan-A(MART-1), and synaptophysin
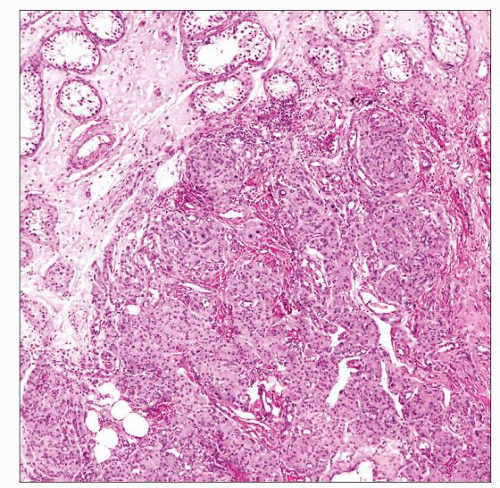 TTAGS shows a well-circumscribed nodule composed of cells with abundant eosinophilic cytoplasm similar to that of a Leydig cell tumor. (Courtesy R. H. Young, MD.) |
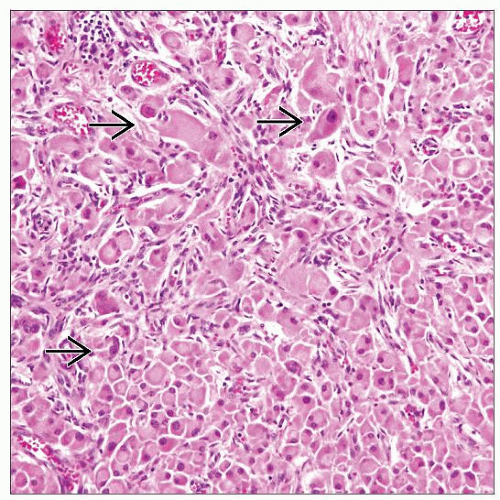 This TTAGS is composed of large polygonal cells with abundant eosinophilic cytoplasm. Random cells show nuclear pleomorphism  . Multifocality and bilaterality are common. (Courtesy R. H. Young, MD.) . Multifocality and bilaterality are common. (Courtesy R. H. Young, MD.) |
TERMINOLOGY
Abbreviations
Testicular “tumor” of adrenogenital syndrome (TTAGS)
Synonyms
Congenital adrenal hyperplasia
Definitions
Benign bilateral testicular lesions in patients with congenital adrenal hyperplasia leading to growth of adrenal-like cells in testis that resemble Leydig cell tumor
Bilaterality, multifocality, and response to medical treatment argue against this being a neoplastic lesion
ETIOLOGY/PATHOGENESIS
Developmental Anomaly
21-hydroxylase deficiency (most common)
Other associated conditions
11-hydroxylase deficiency
Cushing disease
Addison disease
Idiopathic enzyme defect
Cellular origin uncertain; hilar pluripotential cells, adrenal cortical rest cells, Leydig cells are possible candidates
CLINICAL ISSUES
Epidemiology
Incidence
Rare; a few dozen cases reported
Age
Children to early adult (average: 22.5 years)
Presentation
Bilateral orchialgia (92%)
Testicular masses (2/3 palpable)
Symptoms related to steroid hormone deficiency
Salt-losing form of adrenal disorder in 2/3 and non-salt-losing form in 1/3
Isosexual precocious puberty
Laboratory Tests
Steroid hormone evaluation (increased ACTH)
Tumor markers (AFP, hCG, LDH) to exclude possible germ cell tumor
Treatment
Drugs
Exogenous high-dose corticosteroids are mainstay of medical treatment (pain control and regression of tumor)
Surgical approaches
Tumor enucleation or partial orchiectomy for persistently painful masses and steroid unresponsive lesions in setting of bilaterality
Radical orchiectomy is generally not indicated
Prognosis
Benign lesion, symptoms relieved by steroid therapy or surgery
Very rarely associated with seminoma, and 1 reported case of malignant transformation
IMAGE FINDINGS
Ultrasonographic Findings
Bilateral hypoechoic intraparenchymal infiltrative nodules with variable vascularity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


