60
Special Aspects of Geriatric Pharmacology
CASE STUDY
A 77-year-old man comes to your office at his wife’s insistence. He has had documented moderate hypertension for 18 years but does not like to take his medications. He says he has no real complaints, but his wife remarks that he has become much more forgetful lately and has almost stopped reading the newspaper and watching television. A Mini-Mental State Examination reveals that he is oriented as to name and place but is unable to give the month or year. He cannot remember the names of his three adult children nor three random words (eg, tree, flag, chair) for more than 2 minutes. No cataracts are visible, but he is unable to read standard newsprint without a powerful magnifier. Why doesn’t he take his antihypertensive medications? What therapeutic measures are available for the treatment of Alzheimer’s disease? How might macular degeneration be treated?
Society has traditionally classified everyone over 65 as “elderly,” but most authorities consider the field of geriatrics to apply to persons over 75—even though this too is an arbitrary definition. Furthermore, chronologic age is only one determinant of the changes pertinent to drug therapy that occur in older people. In addition to the chronic diseases of adulthood, the elderly have an increased incidence of many conditions, including Alzheimer’s disease, Parkinson’s disease, and vascular dementia; stroke; visual impairment, especially cataracts and macular degeneration; atherosclerosis, coronary and peripheral vascular disease, and heart failure; diabetes; arthritis, osteoporosis, and fractures; cancer; and incontinence. As a result, the need for drug treatment is great in this age group. And as the average life span approaches (and in some countries, already exceeds) 80, this need will increase dramatically.
When all confounders are accounted for, age itself is still the strongest risk factor for cardiovascular and neurodegenerative diseases and most forms of cancer. Research into the molecular basis of aging has answered a few questions and opened many more. It has long been known that caloric restriction alone can prolong the life span of animals, including mammals. Some evidence suggests that calorically restricted mice also remain healthier for a longer time. Drugs that mimic caloric restriction have been shown to increase lifespan in the nematode Caenorhabditis elegans, as well as other species, including mice. Metformin and rapamycin each increase life span alone and appear to have synergistic effects when given together. Sirtuins, a class of endogenous protein deacetylase enzymes, may be linked to life span in some species, but activators (such as resveratrol) of certain sirtuins have not been shown to prolong life in mice. Assuming that safer alternatives to metformin or rapamycin can be found, should everyone over the age of 40 or 60 years take such a drug? Few would maintain that a simple increase in the years of life—life span—is desirable unless accompanied by an increase in the years of healthy life—“health span.”
Important changes in responses to some drugs occur with increasing age in many individuals. For other drugs, age-related changes are minimal, especially in the “healthy old.” Drug usage patterns also change as a result of the increasing incidence of disease with age and the tendency to prescribe heavily for patients in nursing homes. General changes in the lives of older people have significant effects on the way drugs are used. Among these changes are the increased incidence with advancing age of several simultaneous diseases, nutritional problems, reduced financial resources, and—in some patients—decreased dosing adherence (also called compliance) for a variety of reasons. The health practitioner should be aware of the changes in pharmacologic responses that may occur in older people and should know how to deal with these changes.
PHARMACOLOGIC CHANGES ASSOCIATED WITH AGING
In the general population, measurements of functional capacity of most of the major organ systems show a decline beginning in young adulthood and continuing throughout life. As shown in Figure 60–1, there is no “middle-age plateau” but rather a linear decrease beginning no later than age 45. However, these data reflect the mean and do not apply to every person above a certain age; approximately one third of healthy subjects have no age-related decrease in, for example, creatinine clearance up to the age of 75. Thus, the elderly do not lose specific functions at an accelerated rate compared with young and middle-aged adults but rather accumulate more deficiencies with the passage of time. Some of these changes result in altered pharmacokinetics. For the pharmacologist and the clinician, the most important of these is the decrease in renal function. Other changes and concurrent diseases may alter the pharmacodynamic characteristics of particular drugs in certain patients.
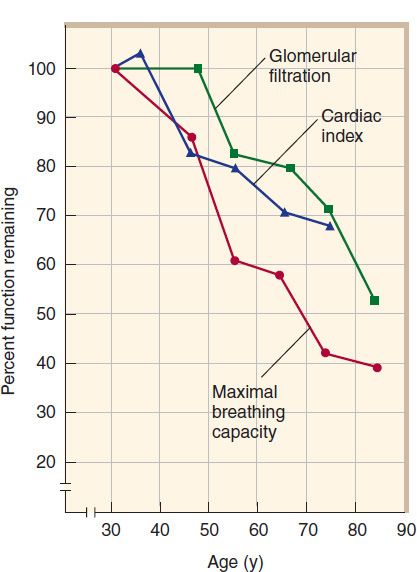
FIGURE 60–1 Effect of age on some physiologic functions. (Adapted, with permission, from Kohn RR: Principles of Mammalian Aging. Copyright © 1978 by Prentice-Hall, Inc. Used by permission of Pearson Education, Inc.)
Pharmacokinetic Changes
A. Absorption
There is little evidence of any major alteration in drug absorption with age. However, conditions associated with age may alter the rate at which some drugs are absorbed. Such conditions include altered nutritional habits, greater consumption of nonprescription drugs (eg, antacids and laxatives), and changes in gastric emptying, which is often slower in older persons, especially in older diabetics.
B. Distribution
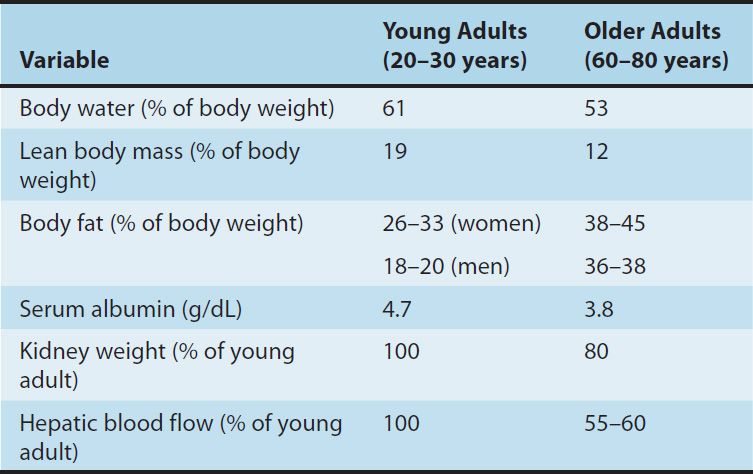
Compared with young adults, the elderly have reduced lean body mass, reduced body water, and increased fat as a percentage of body mass. Some of these changes are shown in Table 60–1. There is usually a decrease in serum albumin, which binds many drugs, especially weak acids. There may be a concurrent increase in serum orosomucoid (α-acid glycoprotein), a protein that binds many basic drugs. Thus, the ratio of bound to free drug may be significantly altered. As explained in Chapter 3, these changes may alter the appropriate loading dose of a drug. However since both the clearance and the effects of drugs are related to the free concentration, the steady-state effects of a maintenance dosage regimen should not be altered by these factors alone. For example, the loading dose of digoxin in an elderly patient with heart failure should be reduced (if used at all) because of the decreased apparent volume of distribution. The maintenance dose may have to be reduced because of reduced clearance of the drug.
TABLE 60–1 Some changes related to aging that affect pharmacokinetics of drugs.
C. Metabolism
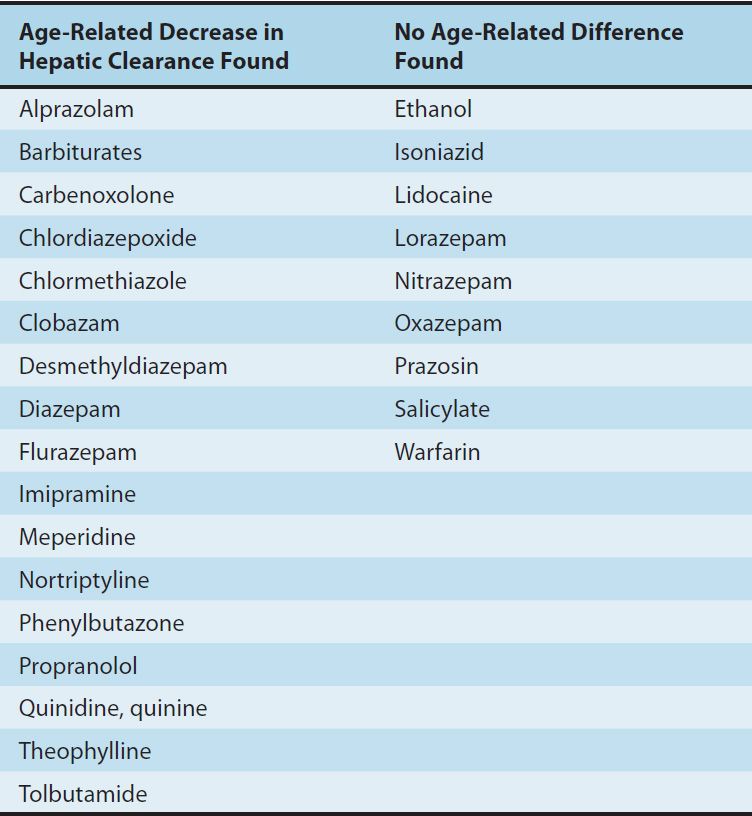
The capacity of the liver to metabolize drugs does not appear to decline consistently with age for all drugs. Animal studies and some clinical studies have suggested that certain drugs are metabolized more slowly in the elderly; some of these drugs are listed in Table 60–2. The greatest changes are in phase I reactions, ie, those carried out by microsomal P450 systems. There are much smaller changes in the ability of the liver to carry out conjugation (phase II) reactions (see Chapter 4). Some of these changes may be caused by decreased liver blood flow (Table 60–1), an important variable in the clearance of drugs that have a high hepatic extraction ratio. In addition, there is a decline with age of the liver’s ability to recover from injury, eg, that caused by alcohol or viral hepatitis. Therefore, a history of recent liver disease in an older person should lead to caution in dosing with drugs that are cleared primarily by the liver, even after apparently complete recovery from the hepatic insult. Finally, malnutrition and diseases that affect hepatic function—eg, heart failure—are more common in the elderly. Heart failure may dramatically alter the ability of the liver to metabolize drugs by reducing hepatic blood flow. Similarly, severe nutritional deficiencies, which occur more often in old age, may impair hepatic function.
TABLE 60–2 Effects of age on hepatic clearance of some drugs.
D. Elimination
Because the kidney is the major organ for clearance of drugs from the body, the age-related decline of renal functional capacity is very important. The decline in creatinine clearance occurs in about two thirds of the population. It is important to note that this decline is not reflected in an equivalent rise in serum creatinine because the production of creatinine is also reduced as muscle mass declines with age; therefore, serum creatinine alone is not an adequate measure of renal function. The practical result of this change is marked prolongation of the half-life of many drugs, and the possibility of accumulation to toxic levels if dosage is not reduced in size or frequency. Dosing recommendations for the elderly often include an allowance for reduced renal clearance. If only the young adult dosage is known for a drug that requires renal clearance, a rough correction can be made by using the Cockcroft-Gault formula, which is applicable to patients from ages 40 through 80:
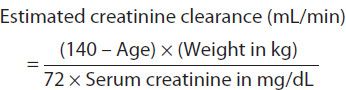
For women, the result should be multiplied by 0.85 (because of reduced muscle mass). It must be emphasized that this estimate is, at best, a population estimate and may not apply to a particular patient. If the patient has normal renal function (up to one third of elderly patients), a dose corrected on the basis of this estimate will be too low—but a low dose is initially desirable if one is uncertain of the renal function in any patient. Simple online calculators using the more modern MDRD (Modification of Diet in Renal Disease) formula are available, eg, http://nkdep.nih.gov/lab-evaluation/gfr-calculators.shtml.
If a precise measure is needed, a standard 12- or 24-hour creatinine clearance determination should be obtained. As indicated above, nutritional changes alter pharmacokinetic parameters. A patient who is severely dehydrated (not uncommon in patients with stroke or other motor impairment) may have an additional marked reduction in renal drug clearance that is completely reversible by rehydration.
The lungs are important for the excretion of volatile drugs. As a result of reduced respiratory capacity (Figure 60–1) and the increased prevalence of active pulmonary disease in the elderly, the use of inhalation anesthesia is less common and intravenous agents more common in this age group. (See Chapter 25.)
Pharmacodynamic Changes
It was long believed that geriatric patients were much more “sensitive” to the action of many drugs, implying a change in the pharmacodynamic interaction of the drugs with their receptors. It is now recognized that many—perhaps most—of these apparent changes result from altered pharmacokinetics or diminished homeostatic responses. Clinical studies have supported the idea that the elderly are more sensitive to some sedative-hypnotics and analgesics. In addition, some data from animal studies suggest actual changes with age in the characteristics or numbers of a few receptors. The most extensive studies suggest a decrease in responsiveness to β-adrenoceptor agonists. Other examples are discussed below.
Certain homeostatic control mechanisms appear to be blunted in the elderly. Since homeostatic responses are often important components of the overall response to a drug, these physiologic alterations may change the pattern or intensity of drug response. In the cardiovascular system, the cardiac output increment required by mild or moderate exercise is successfully provided until at least age 75 (in individuals without obvious cardiac disease), but the increase is the result primarily of increased stroke volume in the elderly and not tachycardia, as in young adults. Average blood pressure goes up with age (in most Western countries), but the incidence of symptomatic orthostatic hypotension also increases markedly. It is thus particularly important to check for orthostatic hypotension on every visit. Similarly, the average 2-hour postprandial blood glucose level increases by about 1 mg/dL for each year of age above 50. Temperature regulation is also impaired, and hypothermia is poorly tolerated by the elderly.
Behavioral & Lifestyle Changes
Major changes in the conditions of daily life accompany the aging process and have an impact on health. Some of these (eg, forgetting to take one’s pills) are the result of cognitive changes associated with vascular or other pathology. One of the most important changes is the loss of a spouse. Others relate to economic stresses associated with greatly reduced income and, frequently, increased expenses due to illness.
 MAJOR DRUG GROUPS
MAJOR DRUG GROUPS
CENTRAL NERVOUS SYSTEM DRUGS
Sedative-Hypnotics
The half-lives of many benzodiazepines and barbiturates increase by 50–150% between ages 30 and 70. Much of this change occurs during the decade from 60 to 70. For some of the benzodiazepines, both the parent molecule and its metabolites (produced in the liver) are pharmacologically active (see Chapter 22). The age-related decline in renal function and liver disease, if present, both contribute to the reduction in elimination of these compounds. In addition, an increased volume of distribution has been reported for some of these drugs. Lorazepam and oxazepam may be less affected by these changes than the other benzodiazepines. In addition to these pharmacokinetic factors, it is generally believed that the elderly vary more in their sensitivity to the sedative-hypnotic drugs on a pharmacodynamic basis as well. Among the toxicities of these drugs, ataxia and other stability impairments lead to increased falls and fractures.
Analgesics
The opioid analgesics show variable changes in pharmacokinetics with age. However, the elderly are often markedly more sensitive to the respiratory effects of these agents because of age-related changes in respiratory function. Therefore, this group of drugs should be used with caution until the sensitivity of the particular patient has been evaluated, and the patient should then be dosed appropriately for full effect. Unfortunately, studies show that opioids are consistently underutilized in patients who require strong analgesics for chronic painful conditions such as cancer. There is no justification for underutilization of these drugs, especially in the care of the elderly, and good pain management plans are readily available (see Morrison, 2006; Rabow, 2011).
Antipsychotic & Antidepressant Drugs
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


