
18
Shoulder Complex
The shoulder joint complex is composed of three joints—the sternoclavicular, acromioclavicular, and glenohumeral joints (Table 18.1). As a group, they attach the upper limb to the scapula and sternum (Figs. 18.1 and 18.2). The mobility provided by three joints working together gives the shoulder complex a wide range of movement. The extensive mobility in the shoulder joint complex also results from the flexible support provided by numerous muscles, ligaments, and tendons. The bones articulating as part of the shoulder joint complex are the humerus, scapula, clavicle, and sternum.
TABLE 18.1 Joints of the Shoulder Complex
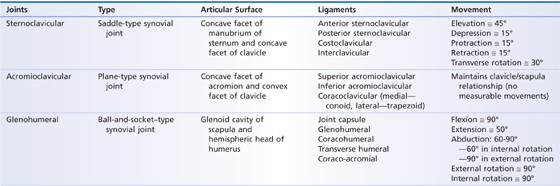
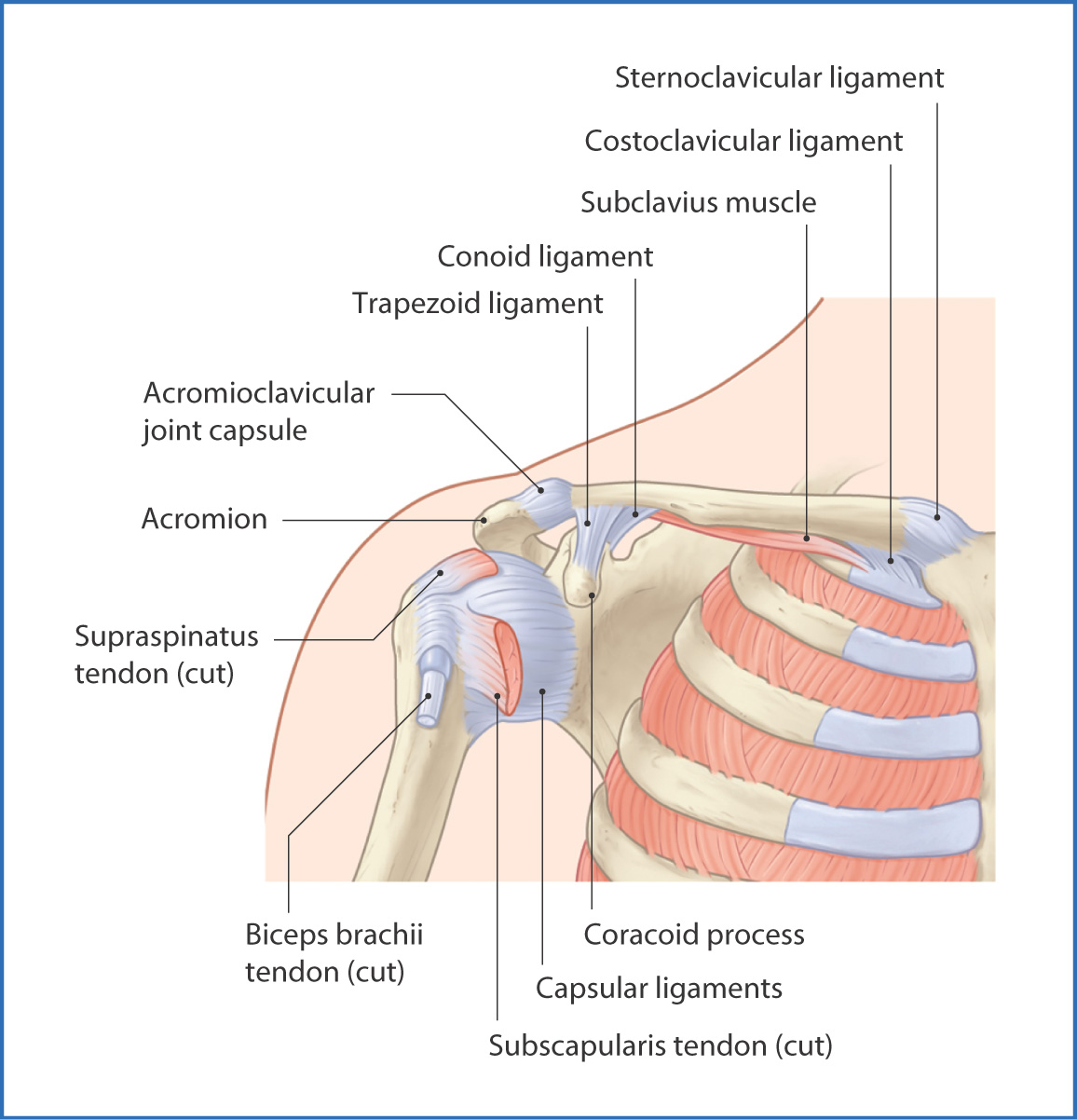
FIGURE 18.1 Glenohumeral joint (anterior view).
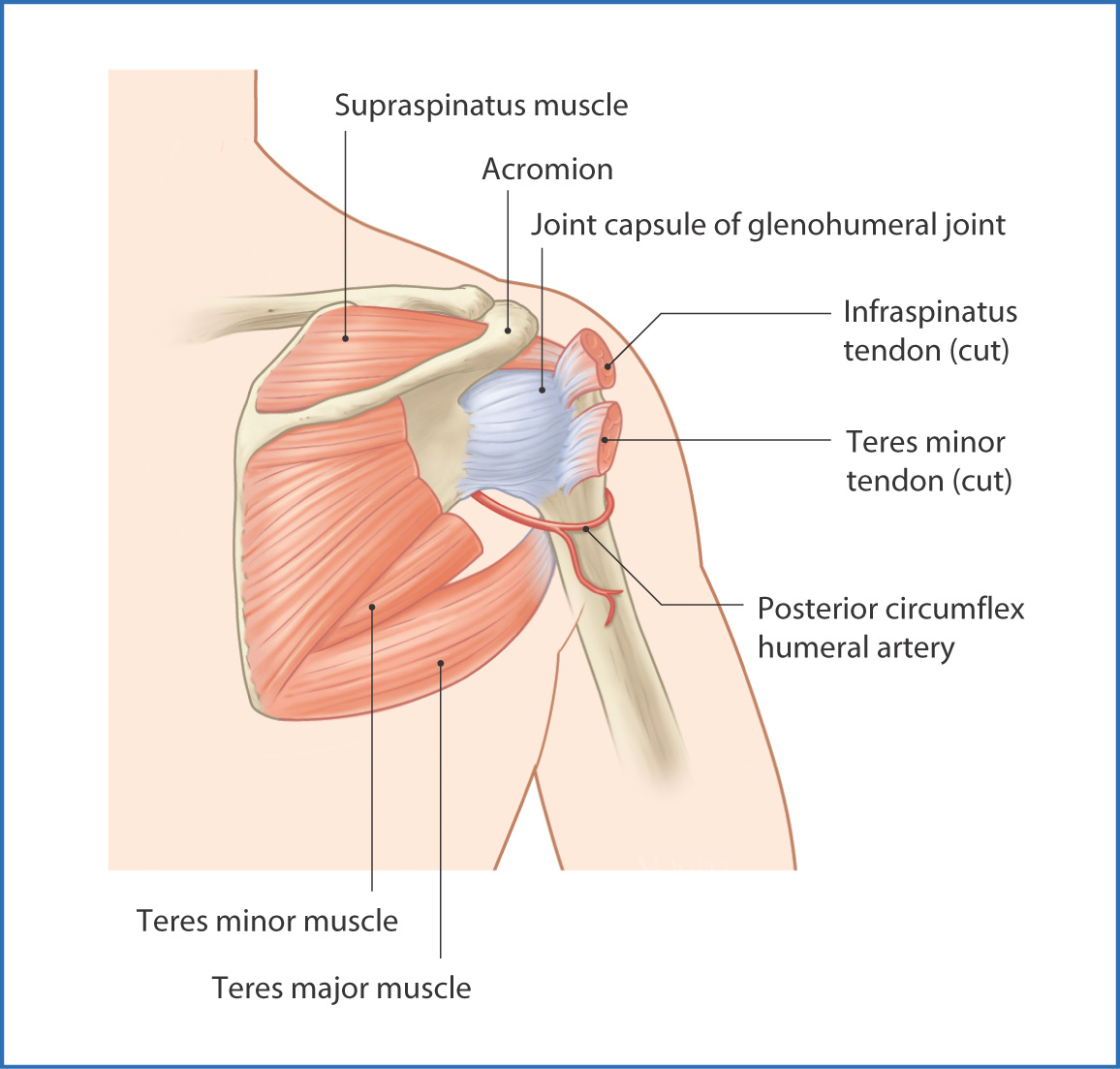
FIGURE 18.2 Glenohumeral joint (posterior view).
Sternoclavicular Joint
The sternoclavicular joint is a saddle-type synovial joint that joins the medial end of the clavicle to the manubrium of the sternum. It is the only point of osseous attachment of the upper limb to the torso. The glenohumeral and acromioclavicular joints join the upper limb to the scapula and clavicle.
Like the acromioclavicular joint (see later), the sternoclavicular joint has a thick fibrous capsule and an articular disc within the joint space. Anterior and posterior sternoclavicular ligaments reinforce the joint capsule. The costoclavicular ligament is a very strong ligament that provides support to the posterior side of the joint as it joins the inferior surface of the medial portion of the clavicle to rib I. An additional interclavicular ligament bridges the space between the clavicles and prevents excessive inferior movement of the clavicle at the sternoclavicular joint.
Innervation of the sternoclavicular joint is provided by branches of the anterior supraclavicular nerves (C3 to C4) and by the subclavian nerve (C5, C6). Blood is supplied by the internal thoracic artery, and venous drainage is to the suprascapular veins. Lymphatic drainage is to the supraclavicular, mediastinal, and axillary lymph nodes.
Acromioclavicular Joint
The acromioclavicular joint connects the acromion of the scapula to the lateral end of the clavicle. It is a plane synovial joint with an articular disc within the joint space. The articular disc increases flexibility. The exterior surface of the joint is completely surrounded by the fibrous joint capsule. The capsule is reinforced superiorly by the superior acromioclavicular ligament and inferiorly by the inferior acromioclavicular ligament. The coracoclavicular ligament, which contains two parts (the lateral trapezoid ligament and the medial conoid ligament), provides the acromioclavicular joint with considerable stability without actually inserting onto the joint.
Innervation to the acromioclavicular joint is from the supraclavicular (C3 to C4), suprascapular, lateral pectoral, and axillary nerves, all of which are components of the brachial plexus (see Chapter 16).
The primary blood supply to the acromioclavicular joint is derived from the suprascapular artery (from the thyrocervical trunk) and the thoraco–acromial artery (from the axillary artery). Venous drainage follows vessels named after the corresponding arteries and is toward the axillary vein. Lymphatic drainage is to the axillary lymph nodes.
Glenohumeral Joint
The glenohumeral joint (commonly referred to as the shoulder joint) is a ball-and-socket synovial joint formed by articulation of the head of the humerus with the glenoid cavity of the scapula. The shallow glenoid cavity is made more bowl-like by a fibrocartilaginous rim—the glenoid labrum. The glenohumeral joint is surrounded by a loose fibrous tissue joint capsule. The glenohumeral ligaments (superior, middle, and inferior) are three thickened areas that form a “Z”-shaped line on the internal surface of the anterior wall of the joint capsule and prevent extreme lateral rotation of the humerus.
Laterally, the band-like coracohumeral ligament originates from the coracoid process of the scapula and inserts onto the superior part of the joint capsule and the anatomical neck of the humerus next to the greater tubercle. The joint capsule is thickened by the transverse humeral ligament and is protected superiorly by the arching of the coraco–acromial ligament.
The head of the humerus is held in the glenoid cavity by four scapular muscles commonly referred to as the rotator cuff muscles—the supraspinatus, infraspinatus, teres minor, and subscapularis muscles.
The suprascapular, axillary, and subscapular nerves innervate the glenohumeral joint and branch to form small nerve branches to the joint as they pass en route to the muscles that they innervate.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


