http://evolve.elsevier.com/McCuistion/pharmacology
Each day, over 1 million new cases of sexually transmitted infection (STI) occur worldwide. The incidence of STIs has been increasing since 2013. Young adults are at risk, particularly young women, but infections among men are also rising. Over 30 bacteria, viruses, and parasites can cause STIs. The most common bacterial pathogens are Chlamydia, Neisseria gonorrhoeae, and Treponema pallidum (syphilis); Trichomonas is a common parasite; and the most common viral pathogens are hepatitis B virus (HBV), herpes simplex virus (HSV), human immunodeficiency virus (HIV), and human papillomavirus (HPV). The majority of persons with STIs experience few or no symptoms, making it difficult to diagnose and treat to stop the spread of infections. STIs are spread through sexual contact, via blood or blood products, and through mother-to-child transmission during pregnancy and childbirth.
Sexually Transmitted Infections
Sexual transmission of pathogens can occur through breaks in the vaginal or cervical mucosa or in the skin covering the shaft or glans of the penis. Each act of coitus results in tiny, friction-induced fissures on these surfaces. Seminal fluid, spermatozoa, vaginal secretions, blood, and other body fluids can carry pathogens. Skin and mucosal lesions can be penetrated by microorganisms, and skin and mucosa can shed microorganisms.
Sexual contact can involve transmission of pathogens through the skin or mouth and via oral-genital, oral-anal, or hand-anal transmission of pathogens through breaks in the skin or mucosal surfaces or from inoculation by infectious body fluids. Anal penetration is particularly risky because of the likelihood of tissue trauma that results in the partner’s exposure to enteric microorganisms. The risk for contracting an STI increases with substance abuse, imprisonment, sexual activity with a partner who has been imprisoned, sexual activity with individuals being paid for sex acts, and rape or sexual assault.
Patients who engage in sexual activity with multiple partners are at high risk for transmission of STIs, particularly HIV. The Centers for Disease Control and Prevention (CDC) reports the risk for getting STIs is markedly increased among individuals who have more than one sexual partner per year versus those who have fewer partners. It should be noted that 5.2% of men between the ages of 15 and 44 report having 5 or more partners in a 12-month period, and 2% of women report the same. Additionally, 21.8% of men between the ages of 15 and 44 report having had 15 or more sexual partners, and 10.6% of women report the same.
Other high-risk practices are anal or vaginal intercourse without a condom, hand-anal contact, contact with menstrual blood during sexual activity, use of an enema before anal intercourse, and urination on broken skin or inside the body. Refer to Fig. 54.1 for guidelines provided by the CDC on the prevention of STIs.
STIs are often manifested as multiple infections. Individuals undergoing treatment for one STI should be assessed for others, including HIV. This is especially true if genital or perianal ulcerations are present.
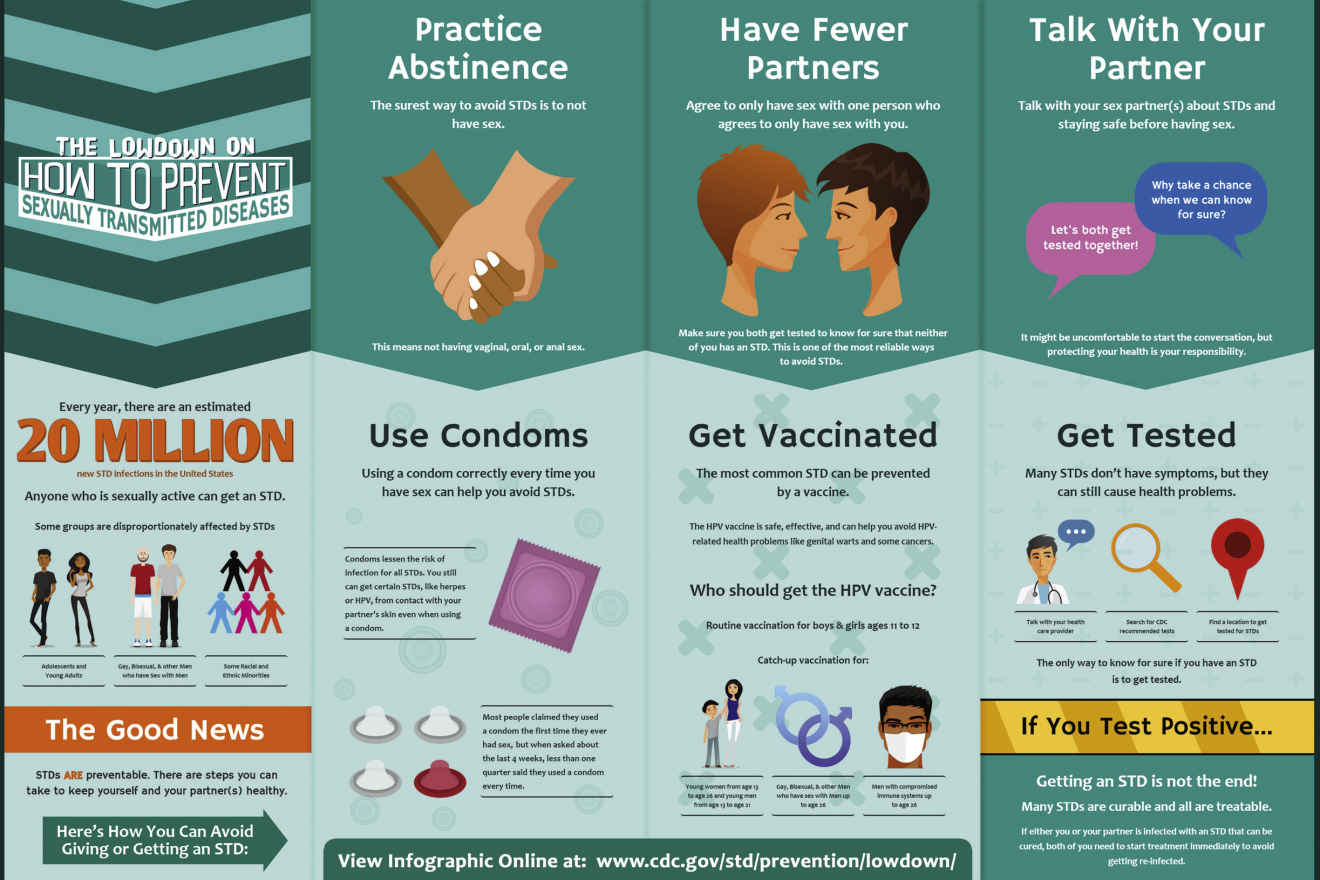
FIG. 54.1 How to Prevent Sexually Transmitted Infections.
From Centers for Disease Control and Prevention. (2016). How you can prevent sexually transmitted diseases. Retrieved from www.cdc.gov/std/prevention
Vertical transmission is the passage of infecting organisms from mother to neonate. Microbes can travel up the reproductive tract from the vagina or cervix and enter the intrauterine environment. Organisms that are of little consequence to healthy adults can be devastating to a fetus. Transmission can also occur through contact with the mother’s blood at birth or through breast milk, as in the case of HIV and HBV. Many STIs, such as syphilis, are transmitted through the placenta and membranes. Others, such as the herpes simplex virus type 2 (HSV-2), require actual contact by the infant with microorganisms in the birth canal. Because of the risk for blindness caused by Chlamydia trachomatis and N. gonorrhoeae, erythromycin ointment is routinely administered in the eyes of neonates as prophylaxis. This is usually done within the first hour after birth.
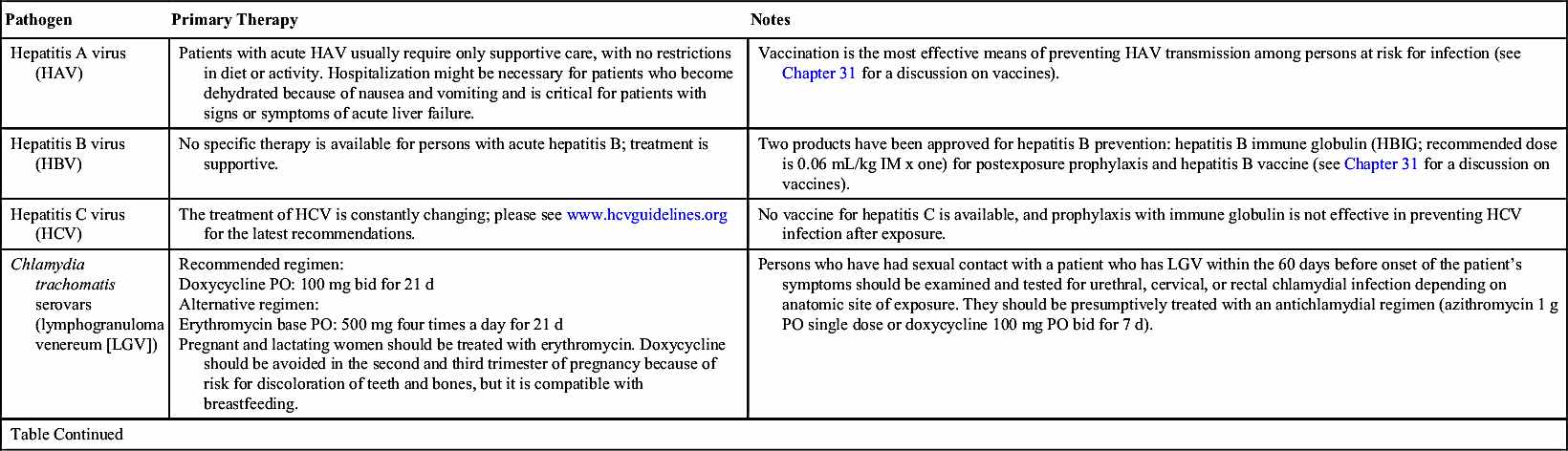
CDC guidelines for the primary treatment of some STI pathogens are listed in Table 54.1; the most common pathogens are discussed in the following section. All sexual contacts of an infected individual should be informed of the exposure so they can be treated. Partners should refrain from sexual activity until each is clear of infection on follow-up evaluation or, at the very least, condoms should be used until each is clear of infection.
Sexually Transmitted Pathogens
The information in this chapter comes directly from the 2015 treatment guidelines for sexually transmitted infections, available at www.cdc.gov/std/tg2015/default.htm.
Bacterial Pathogens
Sexually transmitted bacterial pathogens can be effectively treated with antibiotic therapy. When present, common symptoms include vaginal discharge, urethral discharge or burning (in men), genital ulcers, and abdominal pain.
Bacterial Vaginosis
Bacterial vaginosis (BV) causes a large amount of homogenous, thin, white vaginal discharge with a strong fishy odor. In BV, normal, healthy bacteria in the vagina—lactobacilli—are replaced with anaerobic bacteria, most commonly Gardnerella vaginalis, Mycoplasma hominis, Ureaplasma urealyticum, or Prevotella, Porphyromonas, Bacteroides, Peptostreptococcus, and Mobiluncus species. BV can be transmitted via sexual contact but is not considered an STI; however, having BV can increase a woman’s risk for getting an STI due to the imbalance in vaginal bacteria.
BV is treated with metronidazole 500 mg by mouth (PO) twice a day for 7 days. Because metronidazole can cause stomach upset, it should be taken with food or a full glass of water or milk. Alcohol causes severe nausea and vomiting when ingested with metronidazole, so patients should be instructed not to drink alcoholic beverages or use products that contain alcohol, such as mouthwash, for the duration of drug therapy and for 48 hours after treatment.
Vaginal preparations are also effective in treating BV, such as metronidazole gel 0.75%, one 5-g applicator intravaginally at bedtime for 5 nights; clindamycin cream 2%, one 5-g applicator intravaginally at bedtime for 5 days; or clindamycin ovules, 100 mg intravaginally at bedtime for 3 days.
Oral drugs that are alternatives to metronidazole include tinidazole, either 2 g orally once a day for 2 days or 1 g orally once a day for 5 days, or clindamycin 300 mg orally twice a day for 7 days. Tinidazole has the same precautions with alcohol as metronidazole and should be taken with food. Tinidazole causes slightly less gastrointestinal (GI) upset than metronidazole. Patients taking clindamycin should be instructed to notify their health care provider if diarrhea develops because it may be an indication of Clostridium difficile–associated diarrhea (CDAD). Treating BV is especially important for pregnant women because of the risk of spontaneous abortion, delivery of premature or low-birthweight babies, or pelvic infection developing after delivery. Metronidazole (oral or intravaginal) or clindamycin (oral) are the drugs of choice in pregnancy, and tinidazole should not be used during the first trimester of pregnancy. None of the drugs should be used by nursing mothers because these drugs are excreted in breast milk.
Chlamydia
Chlamydia trachomatis is the most common STI in the United States in young adults. This infection is most often asymptomatic. Women who contract the infection are at risk for developing pelvic inflammatory disease (PID), ectopic pregnancies, and infertility. Because of this, it is recommended that all sexually active women under the age of 25 be screened annually for C. trachomatis and that all women over 25 be screened based on risk factors.
The CDC recommends azithromycin 1 g orally in a single dose as treatment for C. trachomatis infections or doxycycline 100 mg orally twice a day for 7 days. Alternatively, erythromycin base 500 mg orally four times a day for 7 days, erythromycin ethylsuccinate 800 mg orally four times a day for 7 days, levofloxacin 500 mg orally once daily for 7 days, or ofloxacin 300 mg orally twice a day for 7 days may be given.
Doxycycline is contraindicated in the second and third trimesters of pregnancy. In the case of a chlamydial infection during pregnancy, azithromycin 1 g orally in a single dose is the treatment of choice. Alternatively, amoxicillin 500 mg orally three times a day for 7 days may be given. If neither azithromycin nor amoxicillin is an option, erythromycin may be used.
Neonates may contract C. trachomatis from exposure to the mother’s infected cervix during delivery. It most frequently presents as conjunctivitis that develops 5 to 12 days after delivery; however, C. trachomatis can also cause pneumonia in infants between 1 and 3 months old. Prenatal screening and treatment is the best means of prevention. Erythromycin ophthalmic ointment, administered to prevent gonococcal ophthalmia, may also prevent conjunctivitis caused by C. trachomatis.
Persons treated for Chlamydia infection should be instructed to abstain from sexual intercourse for 7 days after single-dose therapy or until a 7-day regimen is completed. Partners should be treated if they had sexual contact during the 60 days preceding the onset of symptoms or diagnosis.
Gonorrhea
In the United States, gonorrhea is the second most common communicable disease. In men, infection by N. gonorrhoeae causes a greenish yellow or whitish discharge from the penis, accompanied by burning with urination. These symptoms usually prompt them to seek evaluation and treatment but often not until they have spread the infection to others. In women, N. gonorrhoeae is frequently asymptomatic. Left untreated, women with N. gonorrhoeae infections develop PID, which can cause tubal scarring that leads to ectopic pregnancies and infertility. Oral infections caused by N. gonorrhoeae cause sore throat and trouble swallowing; on examination, the pharynx resembles strep throat.
Because of the development of resistant N. gonorrhoeae, dual drug therapy is recommended with ceftriaxone 250 mg given intramuscularly (IM) in a single dose plus azithromycin 1 g orally in a single dose for uncomplicated urogenital infections or oral infections. If ceftriaxone is not available, cefixime 400 mg orally in a single dose plus azithromycin 1 g orally in a single dose may be given. Use of two drugs improves treatment efficacy and slows the development of drug resistance.
For those who are allergic to cephalosporins, gemifloxacin 320 mg orally in a single dose plus azithromycin 2 g orally in a single dose may be used; or, alternatively, gentamicin 240 mg IM in a single dose plus azithromycin 2 g orally in a single dose may be used. Women who are diagnosed with N. gonorrhoeae while pregnant should be treated with ceftriaxone 250 mg in a single IM dose and azithromycin 1 g orally as a single dose. Children under 45 kg should receive 25 to 50 mg/kg intravenously (IV) or IM, not to exceed 125 mg IM in a single dose.
Neonates may contract N. gonorrhoeae from exposure to the mother’s infected cervix during delivery. The infection most frequently presents as an acute illness that develops 2 to 5 days after delivery. Prenatal screening and treatment is the best means of prevention, and most states require neonates to be administered erythromycin (0.5%) ophthalmic ointment in each eye in a single application at birth to prevent conjunctivitis caused by N. gonorrhoeae.
Persons receiving treatment for gonorrhea should be instructed to abstain from sexual activity for 7 days after treatment. Persons diagnosed with gonorrhea should also be tested for Chlamydia, syphilis, and HIV. Partners should be treated if they had sexual contact during the 60 days preceding the onset of symptoms or diagnosis.
Syphilis
Syphilis is caused by the bacteria Treponema pallidum; if not treated early in the infectious process, it produces systemic disease that can be fatal. The disease is divided into three stages: primary, secondary, and tertiary.
Primary syphilis infections present with a sore, or chancre, at the site where the infection entered the body—typically, the penis in men and outer genitals or inner vagina in women. It is usually painless. The chancre develops about 3 weeks after exposure and resolves in 3 to 6 weeks without treatment. During this stage, the person is very contagious, even after the chancre has resolved.
Secondary syphilis is characterized by a skin rash that appears 2 to 8 weeks after the chancre. It may occur anywhere on the body, commonly on the hands and soles of the feet; the rash usually does not itch. Mucocutaneous lesions, fever, fatigue, sore throat, and lymphadenopathy may occur as well. The rash usually resolves in about 2 months. During this stage, the person remains very contagious, even after the rash has resolved. After the rash has resolved, a period that lasts anywhere from 1 year to 20 years goes by without any symptoms. This is called the latent stage, and it occurs in persons who have gone untreated. A person may remain contagious during the latent period, and diagnosis can only be made through blood testing.
Tertiary syphilis may occur as early as 1 year after infection or at any time during an untreated person’s lifetime. Large sores inside the body or on the skin occur in the tertiary stage, along with cardiovascular and ocular syphilis and neurosyphilis. Examination of the cerebral spinal fluid (CSF) should be done in persons in the tertiary stage to determine neurologic involvement, even in the absence of clinical neurologic findings.
To diagnose syphilis, two types of serologic testing are necessary to avoid false positives. One test should be a nontreponemal antibody test (e.g., Rapid Plasma Reagin [RPR] or Venereal Disease Research Laboratory [VDRL]) that tests for antibodies produced when a person has syphilis, although it may be produced in other diseases as well (e.g., Lyme disease or malaria). The other test should be a treponemal antibody test (e.g., fluorescent treponemal antibody absorption [FTA-ABS] or T. pallidum particle agglutination assay [TP-PA]), a test for antibodies that specifically target T. pallidum.
Treatment for primary and secondary syphilis is benzathine penicillin G, 2.4 million units given IM in one dose. Infants and children should be treated with benzathine penicillin G 50,000 units/kg IM up to the adult dose of 2.4 million units in a single dose, and these patients should be followed by a pediatric infectious disease specialist.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


