http://evolve.elsevier.com/McCuistion/pharmacology/
Parkinson’s disease is a chronic, progressive, neurologic disorder that affects the extrapyramidal motor tract, which controls posture, balance, and locomotion. Parkinson’s disease is the most common form of parkinsonism, which is considered a syndrome, or a combination of similar symptoms, because of its major features: rigidity (abnormal increased muscle tone), bradykinesia (slow movement), gait disturbances, and tremors. Rigidity increases with movement. Postural changes caused by rigidity and bradykinesia include the chest and head thrust forward with the knees and hips flexed, a shuffling gait, and the absence of arm swing. Other characteristic symptoms are masked facies (no facial expression), involuntary tremors of the head and neck, and pill-rolling motions of the hands. The tremors may be more prevalent at rest.
Alzheimer disease is a chronic, progressive, neurodegenerative condition with marked cognitive dysfunction. Various theories exist as to the cause of Alzheimer disease, with neuritic plaques, degeneration of the cholinergic neurons, and deficiency in acetylcholine among them.
Parkinson’s Disease
In 1817, Dr. James Parkinson described six patients as having “shaking palsy.” Three symptoms were described by Parkinson: (1) involuntary tremors of the limbs, (2) rigidity of muscles, and (3) slowness of movement. In the United States, approximately one million people have Parkinson’s disease, and 60,000 new cases are diagnosed each year. Because Parkinson’s disease generally affects patients 50 years of age and older, many consider the health problem to be part of the aging process caused by loss of neurons. The cardinal symptoms are rigidity, tremors, gait disturbance, and bradykinesia. Normally the symptoms have a gradual onset and are usually mild and unilateral in the beginning.
There are different types of parkinsonism. Pseudoparkinsonism frequently occurs as an adverse reaction to chlorpromazine, haloperidol, lithium, metoclopramide, methyldopa, and reserpine. In addition, parkinsonism symptoms could result from poisons, such as carbon monoxide and manganese, or from disorders, such as arteriosclerosis, encephalitis, infections, stroke, trauma, or Wilson disease (hepatolenticular degeneration). Parkinson’s disease is the most common type, which is a degeneration of dopaminergic neurons leading to a lack of dopamine.
Nonpharmacologic Measures
Symptoms of Parkinson’s disease can be lessened through the use of nonpharmacologic measures such as patient teaching, exercise, nutrition, and group support. Exercise can improve mobility and flexibility; the patient with Parkinson’s disease should enroll in a therapeutic exercise program tailored to this disorder. A balanced diet with fiber and fluids helps prevent constipation and weight loss. Patients with Parkinson’s disease and their family members should be encouraged to attend a support group to help cope with and understand this disorder.
Pathophysiology
Parkinson’s disease is caused by an imbalance of the neurotransmitters dopamine and acetylcholine, and it is marked by degeneration of neurons of the extrapyramidal (motor) tract in the substantia nigra of the midbrain. The reason for the degeneration of neurons is unknown.
The two neurotransmitters within the neurons of the striatum of the brain are dopamine (DA), an inhibitory neurotransmitter, and acetylcholine (ACh), an excitatory neurotransmitter. DA is released from the dopaminergic neurons, and ACh is released from the cholinergic neurons. DA normally maintains control of ACh and inhibits its excitatory response. In Parkinson’s disease, an unexplained degeneration of the dopaminergic neurons occurs, and an imbalance between DA and ACh results. With less DA production, the excitatory response of ACh exceeds the inhibitory response of DA. An excessive amount of ACh stimulates neurons that release gamma-aminobutyric acid (GABA). With increased stimulation of GABA, the symptomatic movement disorders of Parkinson’s disease occur.
By the time early symptoms of Parkinson’s disease appear, 80% of the striatal dopamine has already been depleted. The remaining striatal neurons synthesize DA from levodopa and release DA as needed. Before the next dose of levodopa, symptoms such as slow walking and loss of dexterity return or worsen, but within 30 to 60 minutes of receiving a dose, the patient’s functioning is much improved.
Drugs used to treat Parkinson’s disease replace the dopamine deficit and reduce the symptoms. These drugs fall into five categories: (1) anticholinergics, which block cholinergic receptors; (2) dopamine replacements, which stimulate DA receptors; (3) dopamine agonists, which stimulate DA receptors; (4) monoamine oxidase B (MAO-B) inhibitors, which inhibit the MAO-B enzyme that interferes with DA; and (5) catechol-O-methyltransferase (COMT) inhibitors, which inhibit the COMT enzyme that inactivates DA. Table 20.1 compares the various drugs for Parkinson’s disease.
Anticholinergics
Anticholinergic drugs reduce the rigidity and some of the tremors characteristic of Parkinson’s disease but have a minimal effect on bradykinesia. The anticholinergics are parasympatholytics that inhibit the release of acetylcholine. Anticholinergics are still used to treat drug-induced parkinsonism, or pseudoparkinsonism, a side effect of the antipsychotic phenothiazine drug group. Examples of anticholinergics used for Parkinson’s disease include trihexyphenidyl and benztropine.
 Nursing Process: Patient-Centered Collaborative Care
Nursing Process: Patient-Centered Collaborative CareAntiparkinson Anticholinergic Agents
Assessment
• Obtain a health history. Report any history of glaucoma, gastrointestinal (GI) dysfunction, urinary retention, angina, or myasthenia gravis. All anticholinergics are contraindicated if a patient has glaucoma.
• Obtain a drug history. Report any probable drug-drug interactions, such as with phenothiazines, tricyclic antidepressants (TCAs), and antihistamines, which increase the effect of trihexyphenidyl.
• Assess baseline vital signs for future comparisons. The pulse rate may increase.
• Assess the patient’s knowledge regarding the medication regimen.
• Determine usual urinary output as a baseline for comparison. Urinary retention may occur with continuous use of anticholinergics.
Nursing Diagnoses
• Mobility, Impaired Physical related to muscle rigidity, tremors, and bradykinesia
• Elimination, Impaired Urinary related to urinary retention
• Knowledge, Deficient related to unfamiliarity with drug regimen
Planning
• Patient will have decreased involuntary symptoms caused by Parkinson’s disease or drug-induced parkinsonism.
Nursing Interventions
• Monitor vital signs, urine output, and bowel sounds. Increased pulse rate, urinary retention, and constipation are side effects of anticholinergics.
• Observe for involuntary movements.
Patient Teaching
General
• Advise patients to avoid alcohol, cigarettes, caffeine, and aspirin to decrease gastric acidity.
Side Effects
• Encourage patients to relieve a dry mouth with hard candy, ice chips, or sugarless chewing gum. Anticholinergics decrease salivation.
• Suggest that patients use sunglasses in direct sunlight because of possible photophobia.
• Advise patients to void before taking the drug to minimize urinary retention.
•  Counsel patients who take an anticholinergic for control of symptoms of Parkinson’s disease to have routine eye examinations because anticholinergics are contraindicated in patients with glaucoma.
Counsel patients who take an anticholinergic for control of symptoms of Parkinson’s disease to have routine eye examinations because anticholinergics are contraindicated in patients with glaucoma.
Counsel patients who take an anticholinergic for control of symptoms of Parkinson’s disease to have routine eye examinations because anticholinergics are contraindicated in patients with glaucoma.Diet
• Encourage patients to ingest foods high in fiber and to increase fluid intake to prevent constipation.
 Cultural Considerations
Cultural Considerations• Assess personal beliefs of patients and family, and modify communications to meet cultural needs; use an interpreter and community nurse follow-up as needed.
Evaluation
• Evaluate the patient’s response to trihexyphenidyl or benztropine mesylate to determine whether Parkinson’s disease symptoms are controlled.
Table 20.2 lists the anticholinergics and their dosages, uses, and considerations. Anticholinergics used to treat Parkinson’s disease are also discussed in Chapter 16.
Dopaminergics
Carbidopa and Levodopa
The first dopaminergic drug was levodopa, which was introduced in 1961 but is no longer available in the United States. When introduced, levodopa was effective in diminishing symptoms of Parkinson’s disease and increasing mobility; this is because the blood-brain barrier admits levodopa but not dopamine. The enzyme dopa decarboxylase converts levodopa to dopamine in the brain, but this enzyme is also found in the peripheral nervous system and allows 99% of levodopa to be converted to dopamine before it reaches the brain. Therefore only about 1% of levodopa taken is available to be converted to dopamine once it reaches the brain, and large doses are needed to achieve a pharmacologic response. These high doses could cause many side effects, including nausea, vomiting, dyskinesia, orthostatic hypotension, cardiac dysrhythmias, and psychosis.
Because of the side effects of levodopa and the fact that so much levodopa is metabolized before it reaches the brain, an alternative drug, carbidopa, was developed to inhibit the enzyme dopa decarboxylase. By inhibiting the enzyme in the peripheral nervous system, more levodopa reaches the brain. The carbidopa is combined with levodopa in a ratio of 1 part carbidopa to 10 parts levodopa. Fig. 20.1 illustrates the comparative action of levodopa and carbidopa-levodopa.
The advantages of combining levodopa with carbidopa are that more dopamine reaches the basal ganglia and that smaller doses of levodopa are required to achieve the desired effect. The disadvantage of the carbidopa-levodopa combination is that with more available levodopa, more side effects may occur, which may include nausea, vomiting, dystonic movement (involuntary abnormal movement), and psychotic behavior. The peripheral side effects of levodopa are not as prevalent; however, angioedema, palpitations, and orthostatic hypotension may occur. Prototype Drug Chart 20.1 lists the pharmacologic behavior of carbidopa-levodopa.
TABLE 20.2
Antiparkinson Drugs: Anticholinergics
| Drug | Route and Dosage | Uses and Considerations |
| Benztropine mesylate | Parkinson’s disease: A: PO/IM: Initially 0.5-1 mg/d at bedtime; maint: 0.5-6 mg/d; max: 8 mg/d Drug-induced parkinsonism: A: IV/IM/PO: 1-4 mg qd/bid | For Parkinson’s disease, tremor, and drug-induced parkinsonism. Contraindicated in glaucoma and dementia. May cause blurred vision, ocular hypertension, weakness, dry mouth, nausea, constipation, anhidrosis, and urinary retention. Pregnancy category: C∗: PB: UK; t½: UK |
| Trihexyphenidyl hydrochloride | Parkinson’s disease: A: PO: Initially 1 mg, then increase by 2 mg q3-5d; maint: 6-10 mg/d; max: 15 mg/d Extended release: A: PO: 5-10 mg after breakfast or in 2 divided doses 12 h apart Drug-induced parkinsonism: A: PO: Initially 1 mg; maint: 5-15 mg/d | For Parkinson’s disease and drug-induced pseudoparkinsonism. May cause dizziness, drowsiness, increased intraocular pressure, anxiety, headache, insomnia, weakness, paresthesia, dry mouth, nausea, vomiting, constipation, restlessness, and urinary retention. Pregnancy category: C∗; PB: UK; t½: UK |
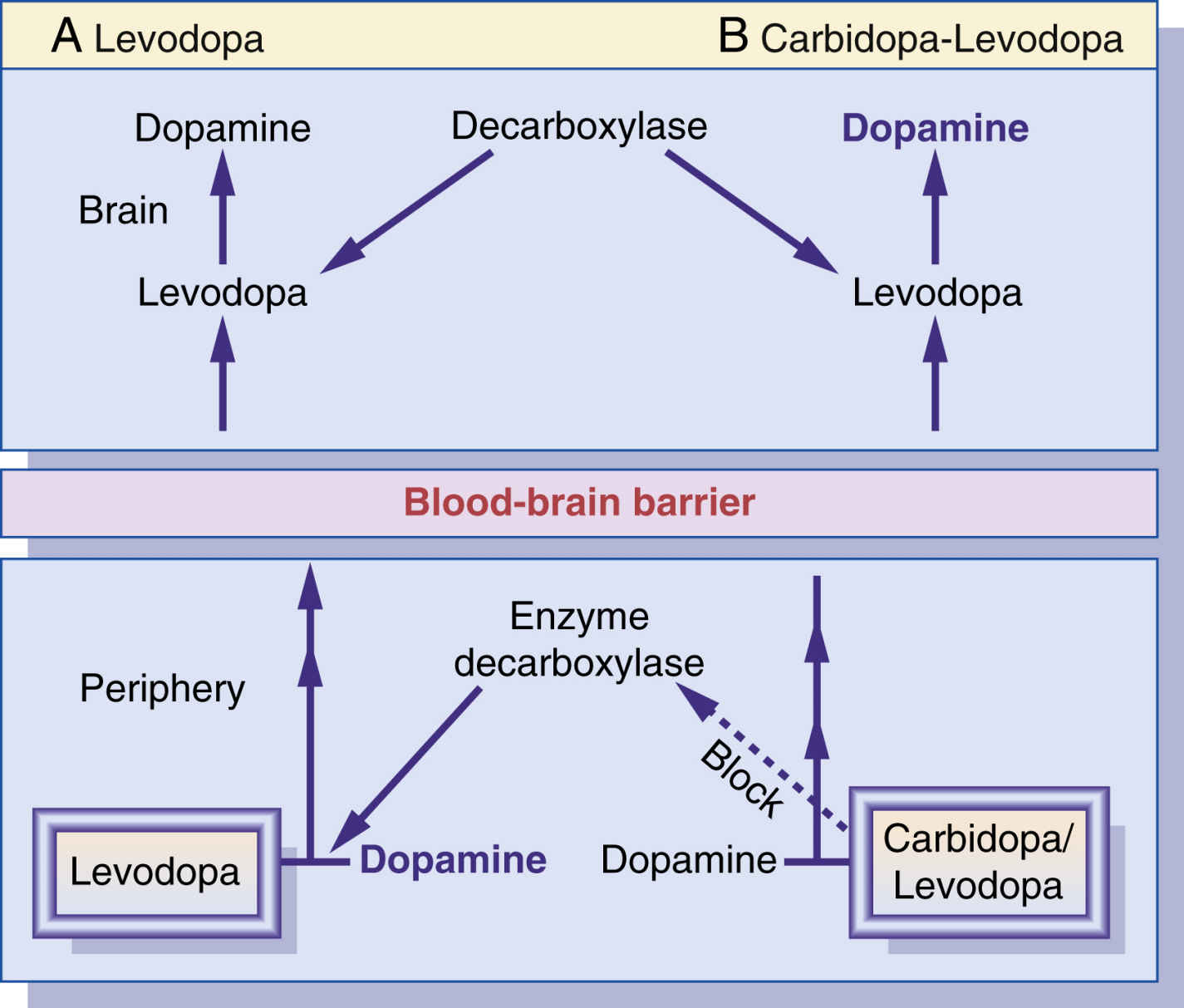
FIG. 20.1 A, When levodopa is used alone, only 1% reaches the brain because 99% converts to dopamine while in the peripheral nervous system. B, By combining carbidopa with levodopa, carbidopa can inhibit the enzyme decarboxylase in the periphery, thereby allowing more levodopa to reach the brain.
 Nursing Process: Patient-Centered Collaborative Care
Nursing Process: Patient-Centered Collaborative CareAntiparkinson Dopaminergic Agents: Carbidopa-Levodopa
Assessment
• Obtain vital signs to use for future comparisons.
• Assess patients for signs and symptoms of Parkinson’s disease, including stooped forward posture, shuffling gait, masked facies, and resting tremors.
• Obtain a patient history that includes glaucoma, heart disease, peptic ulcers, kidney or liver disease, and psychosis.
• Obtain a drug history. Report if drug-drug interaction is probable. Drugs that should be avoided or closely monitored are carbidopa-levodopa, bromocriptine, and anticholinergics.
Nursing Diagnoses
• Mobility, Impaired Physical related to dizziness
• Activity Intolerance, Risk for
• Falls, Risk for
• Knowledge, Deficient related to unfamiliar medications
Planning
• Patient’s symptoms of Parkinson’s disease will be decreased or absent after 1 to 4 weeks of drug therapy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


