Risk Factors for Developing Breast Carcinoma
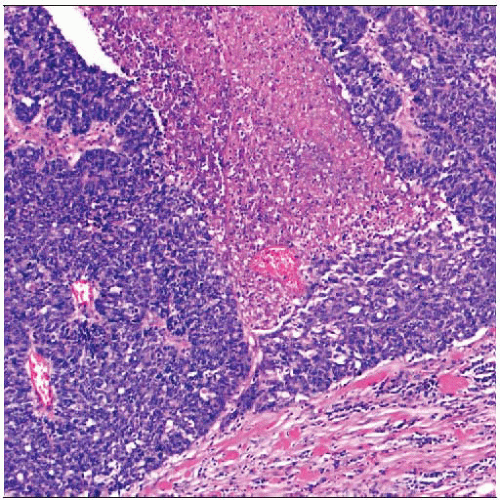 The most important risk factors for young women developing breast cancer are family history and ethnicity. The cancers are frequently poorly differentiated, highly proliferative, and ER negative. |
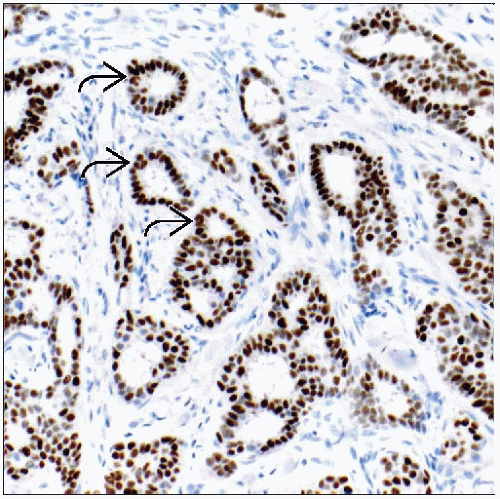 Risk factors for older women are typically associated with estrogen exposure, hormone replacement therapy, and screening. Most common are well- to moderately differentiated ER-positive  cancers. cancers. |
BREAST CANCER RISK
Introduction
Breast cancer is most common non-skin malignancy among women and is 2nd most common cause of cancer death
All women are considered to be at risk, but level of risk varies in population
Lifetime risk of developing invasive breast cancer ranges from 3% (for women without risk factors) to > 80% (for women with highly penetrant germline mutations)
Average lifetime risk of developing breast cancer is 1 in 8 women (approximately 12%)
Measuring degree of risk aids in
Individual choices about risk reduction (e.g., chemoprevention or prophylactic surgery)
Optimal screening strategy
Decisions about testing for single gene mutations
Stratification of patients for enrollment in trials
Providing important clues into cause and biology of breast cancer
Risk factors for developing different molecular types of breast cancer vary and are not yet well understood
Majority of risk factors cannot be modified (e.g., age, gender, ethnicity, family history) or would be very difficult to modify (e.g., age at 1st pregnancy, age at menopause)
Breast Cancer Risk Assessment Tools
Gail and Claus models are among most widely known examples of breast cancer risk assessment tools
Useful to quantify magnitude of risk for individual patients
Not applicable for women who have been diagnosed with DCIS or LCIS
Different models are used for predicting risk for women with BRCA1 or BRCA2 mutations
Do not take into account increased risk due to chest wall radiation
Gail model (http://www.cancer.gov/bcrisktool/) provides risk estimate for the next 5 years and for lifetime
Incorporates patient age (must be 35 or older), ethnicity, age at menarche, age at 1st live birth, number of 1st-degree relatives with invasive breast cancer, number of prior breast biopsies, and diagnosis of atypical hyperplasia
Women with risk of ≥ 1.66% in next 5 years are eligible for chemoprevention with hormonal agents
Claus model uses information about family history
Incorporates patient age, 1st- and 2nd-degree relatives with breast cancer, age of onset in relatives, family history of ovarian cancer
These models perform better for predicting ER-positive cancer than ER-negative cancer
FACTORS ASSOCIATED WITH BREAST CANCER RISK
Gender
Women are at much higher risk than men
Only 1 of every 100 breast cancers occur in males
Most likely due to larger pool of potential cancer precursor cells and estrogenic effects in women
Age
Age-specific incidence rates for breast cancer increase dramatically after age 40
Increase with age is primarily for ER-positive cancers
Peak incidence for breast cancer among women occurs between 75-79 years
Median age at diagnosis in USA: 61 years
Lifetime probability of being diagnosed with breast cancer diminishes as increased age ranges are achieved
Age 30, lifetime risk of breast cancer: 12.5%
Age 50, lifetime risk of breast cancer: 11.1%
Age 70, lifetime risk of breast cancer: 6.6%
Estrogen Exposure
Exposure to higher levels of estrogen increases lifetime risk of developing breast cancer
Factors that reduce risk of breast cancer
Late menarche, early natural menopause, or oophorectomy
Prolonged breastfeeding (4.3% reduction in risk for each year of breastfeeding)
Use of estrogen antagonists such as tamoxifen
Low endogenous estradiol levels
Obesity in premenopausal women
Factors that increase risk of breast cancer
Early menarche and late menopause (early age at menarche [relative risk (RR) = 1.3], late menopause [RR=1.5])
Nulliparity
Obesity in postmenopausal women (elevated estradiol levels compared with women of normal weight)
Adult weight gain and abdominal fatness
Excess body fat may influence steroid hormone levels and inflammatory responses
Hormone replacement therapy (HRT)
After publication of the Women’s Health Initiative trial in 2002, number of women using HRT decreased
Incidence of invasive breast carcinoma and DCIS dropped 10-15% in women over age 50 but not in younger age groups
Decrease occurred for ER-positive cancers
It is not known if HRT causes cancer, increases rate of growth of existing cancers, stimulates angiogenesis, &/or has effects on breast cancer detection
How estrogen exposure increases breast cancer risk is unknown
Estrogen increases mitotic rate of breast cells
Increased mitogenic stimulus may increase the risk of mutation
Estrogen mitogenic drive may act as cancer promoter and contribute to disease progression
Estrogen can act as carcinogen when converted to mutagenic metabolites
Pregnancy
Pregnancy both increases and decreases risk of breast cancer
Transiently increases risk of breast cancer; over many years, risk declines and eventually becomes lower than for nulliparous women (cross-over effect)
For young women (< 20 years), protective effect predominates, and lifetime risk of ER-positive breast cancer is reduced by 1/2
Terminal differentiation of epithelial cells may occur, thus reducing potential pool of cancer precursors
Additional pregnancies further reduce risk (˜ 7% per pregnancy)
Pregnancy permanently changes gene expression profiles of breast tissue
For older women (> 35 years), increased risk predominates and extends for longer period of time
Cancers diagnosed during pregnancy or in postpartum period usually present at higher stages and have poor prognosis
In only 1 of 3,000-10,000 pregnancies is breast cancer diagnosed during or within 1 year
Many proposed mechanisms for the increase in risk
High hormonal levels could stimulate proliferation of precursor lesions, increasing risk of cancer
High hormonal levels may stimulate preexisting cancers to proliferate
However, many pregnancy-associated carcinomas are ER and PR negative
Stroma may become more permissive to allow lobular expansion and branching during pregnancy, which could facilitate progression from carcinoma in situ to invasive carcinoma
Stroma during post-pregnancy involution is similar to that of wound-healing and could promote cancer growth and metastasis
Mammographic Density
Mammographic appearance depends on tissue composition of breast
Stromal tissue and glandular epithelium attenuate x-rays more than fat and increase mammographic density
Mammographic density is strong risk factor for breast cancer
4-5x greater risk in women with density in > 75% of the breast
Density of breast tissue is influenced by age, parity, body mass index, and menopause
Twin studies suggest that % mammographic density, at a given age, is heritable
Hereditary factors may explain up to 63% of variance in breast density
Investigation of gene associated with breast density is an active area of research
Gene profile associated with density may help identify potential targets for breast cancer prevention
Family History
10-20% of patients with breast cancer have a 1st-degree relative with breast cancer
Only 1% have more than 1 affected 1st-degree relative
˜ 50% are thought to be due to heredity and ˜ 50% due to coincidental cases in the same family
Therefore, 5-10% of breast cancer is primarily due to inheritance of susceptibility gene(s)
˜ 4% of hereditary breast cancers are due to a single, highly penetrant gene
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


