Primary Lymphoma
G. Petur Nielsen, MD
Andrew E. Rosenberg, MD
Key Facts
Terminology
Primary lymphoma of bone is defined as lymphoma originating in bone ± extension into adjacent soft tissues
Etiology/Pathogenesis
Most primary bone lymphomas are sporadic and of unknown etiology
Clinical Issues
Usually adults; approximately 50% are > 40 years
Femur is most common location followed by pelvis, vertebrae, and humerus
Approximately 10-40% of cases of lymphoma are multifocal/polyostotic; several lesions in 1 bone or multiple bones involved concurrently
Produces pain, erythema, swelling
Treatment with radiation and chemotherapy of large B-cell lymphoma has 75% 10-year survival
Image Findings
Large, lytic, and destructive
In some cases, tumor may elicit extensive medullary sclerosis
Microscopic Pathology
Diffuse large B-cell lymphoma is most common type by far in both adults and children
Lymphoblastic lymphoma is 2nd most common type to arise in children (40% of cases); uncommon in adults
Anaplastic large cell lymphoma is rare but most common primary T-cell lymphoma of bone
 This lymphoma of bone presents as a permeative, aggressive mass involving the acetabulum, ilium, ischium, and pubic ramus is shown. The tumor also extends into the intrapelvic soft tissues and gluteal muscles. |
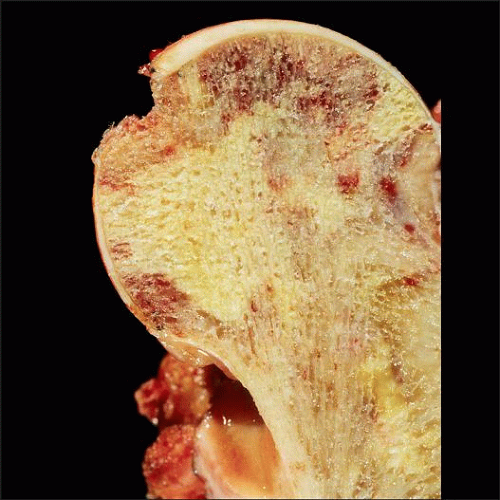 Large B cell lymphoma of the femoral head appears as a geographic zone that is tan-pale yellow and surrounded by hemorrhage. The tumor replaces the marrow and surrounds individual bony trabeculae. |
TERMINOLOGY
Synonyms
Reticulum cell sarcoma (outdated)
Primary non-Hodgkin lymphoma of bone
Definitions
Primary lymphoma originating in bone ± soft tissue extension
Lymphoma should not be identified elsewhere; however, some studies include patients with regional lymph node involvement
No extraosseous distant disease should be identified within 4-6 months of initial diagnosis
Does not include leukemia involving bone
ETIOLOGY/PATHOGENESIS
Etiology
Most primary bone lymphomas are sporadic and of unknown etiology
Rarely reported in patients with HIV, longstanding osteomyelitis, or Paget disease of bone
CLINICAL ISSUES
Epidemiology
Incidence
Rare and accounts for approximately 5% of primary malignant bone tumors and about 5% of all extranodal lymphomas
< 1% of all lymphomas arise in bone with slightly higher incidence in children
Age
Usually adults; approximately 50% are > 40 years; minority arise in children and adolescents
Gender
Slight male predominance
Site
Femur is most common location followed by pelvis, vertebrae, and humerus
Usually arises in metadiaphyseal region
Approximately 10-40% of cases are multifocal (polyostotic), producing several lesions in 1 bone or involving multiple bones concurrently
Presentation
Pain, erythema, swelling
May present with pathologic fracture
Tumors of axial skeleton may cause symptoms related to nerve impingement
10% of patients have constitutional symptoms
More common with polyostotic disease
Fever, anemia, fatigue
Treatment
Currently treated with radiation and chemotherapy
Surgery is indicated for pathologic fracture
Prognosis
10-year disease-free survival rate for large B-cell lymphoma approaches 75%
Lymphomas with follicular center-like immunophenotype may have better prognosis
Prognosis for anaplastic large cell lymphoma is poor
IMAGE FINDINGS
Radiographic Findings
Large, lytic and destructive
May erode cortex and form soft tissue mass
Bone margins are “moth eaten” or permeative
Onion skin periosteal reaction may be present
Because of highly infiltrating growth pattern, soft tissue mass tends to be concentrically distributed around affected bone
In some cases, tumor may elicit extensive medullary sclerosis
Occasionally, findings on plain radiography are minimal with abnormalities only recognized on bone scan, CT, or MR
MR Findings
Provides important information regarding extent of bone and soft tissue involvement
CT Findings
Helpful in identifying extent of disease
MACROSCOPIC FEATURES
General Features
Centered in medullary cavity
May destroy cortex and extend into soft tissue
Moderately firm, gray-white and fleshy, frequently with areas of necrosis
MICROSCOPIC PATHOLOGY
Histologic Features
Exhibits same features as nodal lymphomas and are classified accordingly
Diffuse large B-cell lymphoma is most common type by far in both adults and children
Lymphoblastic lymphoma is 2nd most common type to arise in children (40% of cases)
Anaplastic large cell lymphoma is rare but most common primary T-cell lymphoma of bone
Various other types of lymphomas including Hodgkin lymphoma can rarely arise in bone
Lymphomas frequently contain scattered nonneoplastic small lymphocytes
Because of extensive necrosis or crush artifact that may be present, several biopsies may be required before definitive diagnosis can be rendered
ANCILLARY TESTS
Immunohistochemistry
Immunoprofile varies according to type
Large B-cell lymphomas express leukocyte common antigen (LCA) and B-cell markers
Anaplastic large cell lymphoma may be positive or negative for ALK
ALK(+) tumors mainly affect children whereas ALK(−) tumors affect adults
Lymphoblastic lymphoma may not express LCA and can be CD99(+)
DIFFERENTIAL DIAGNOSIS
Round Cell Lesions
Osteomyelitis, Langerhans cell histiocytosis, Ewing sarcoma/primitive neuroectodermal tumor, metastatic small cell carcinoma, neuroblastoma, rhabdomyosarcoma, and other round cell malignancies
Immunohistochemistry, electron microscopy, and cytogenetic analysis may be necessary to distinguish amongst these possibilities
DIAGNOSTIC CHECKLIST
Pathologic Interpretation Pearls
Think lymphoma if malignant round cell tumor with extensive necrosis or crush artifact
SELECTED REFERENCES
1. Singh T et al: Primary bone lymphoma: a report of two cases and review of the literature. J Cancer Res Ther. 6(3):296-8, 2010
2. Glotzbecker MP et al: Primary non-Hodgkin’s lymphoma of bone in children. J Bone Joint Surg Am. 88(3):583-94, 2006
Image Gallery
Imaging Features
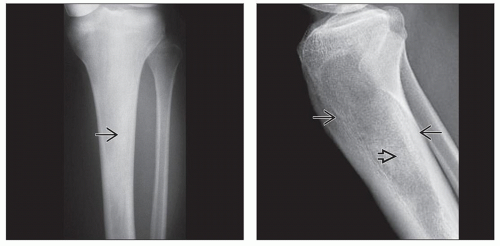 (Left) Radiograph shows lymphoma of bone manifesting as an ill-defined zone of medullary sclerosis  . The cortex is intact with no identifiable periosteal reaction. (Right) Radiograph shows lymphoma of bone of the proximal tibial metaphysis appearing as a poorly defined lytic lesion with endosteal resorption anteriorly and posteriorly . The cortex is intact with no identifiable periosteal reaction. (Right) Radiograph shows lymphoma of bone of the proximal tibial metaphysis appearing as a poorly defined lytic lesion with endosteal resorption anteriorly and posteriorly  . The distal component is indistinct with an area of sclerosis . The distal component is indistinct with an area of sclerosis  . The cortex and periosteum are intact, and there is no soft tissue component. . The cortex and periosteum are intact, and there is no soft tissue component. |
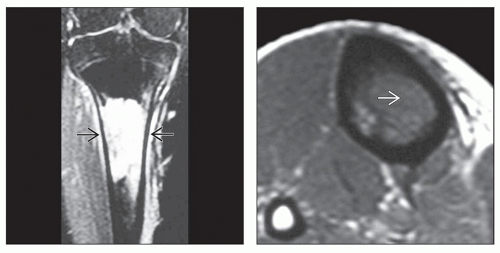 (Left) Fluid-sensitive coronal MR with fat saturation shows that the bone lymphoma replaces the marrow of the proximal tibial diaphysis. The small hyperintense soft tissue component with intact-appearing cortex is a manifestation of the permeative nature of the lesion
 . (Right) Axial T1WI MR shows a lymphoma that has a hypointense signal within the medullary cavity of the tibia . (Right) Axial T1WI MR shows a lymphoma that has a hypointense signal within the medullary cavity of the tibia  . The tumor appears to be confined to the bone, and the cortex seems to be intact. . The tumor appears to be confined to the bone, and the cortex seems to be intact.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|