Plasmacytoma/Myeloma
Vikram Deshpande, MD
G. Petur Nielsen, MD
Andrew E. Rosenberg, MD
Key Facts
Terminology
Plasma cell myeloma is a bone-marrow-based, multifocal plasma cell neoplasm associated with M protein in serum &/or urine
Solitary plasmacytoma of bone is a localized bone tumor consisting of monoclonal plasma cells
Clinical Issues
Most common primary malignant bone tumor
Median age at diagnosis: ˜ 70 years
Most common sites are vertebrae, ribs, skull, pelvis, femur, clavicle, and scapula
Image Findings
Well-circumscribed geographic lytic lesion centered in bone marrow without identifiable matrix
May show multiloculated appearance
Microscopic Pathology
Tumoral mass of plasma cells displacing normal bone marrow elements
Mature plasma cells, plasmablasts, and pleomorphic forms may be seen
Cytoplasmic Ig may produce variety of morphologically distinctive findings, including Mott cells and crystalline rods
Ancillary Tests
Immunohistochemistry &/or in situ hybridization for light chains assist in recognizing monoclonal plasma cell population
Top Differential Diagnoses
Metastatic carcinoma and lymphoma
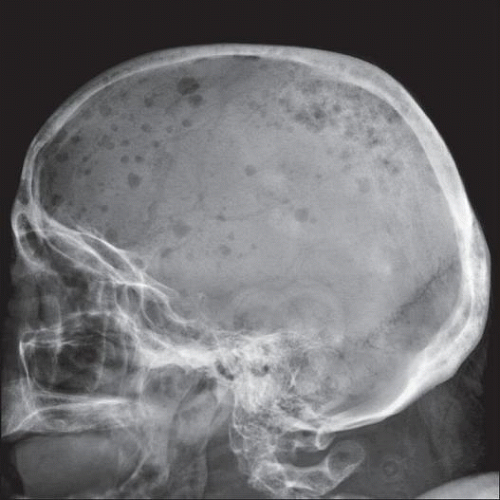 Lateral radiograph of skull shows multiple lytic lesions. Note the small punched-out foci of lucency in the frontal and parietal areas. This is a characteristic appearance of multiple myeloma. |
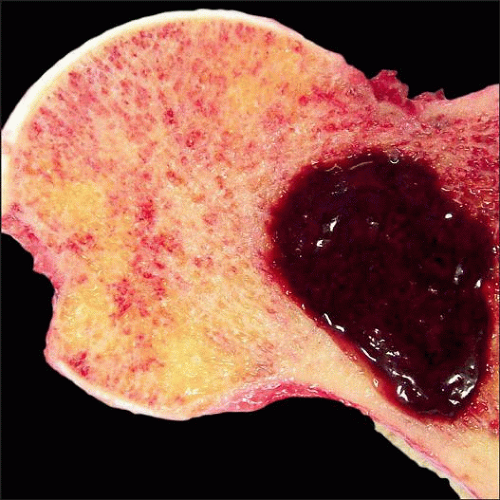 Gross photo shows a resected femoral head involved by plasmacytoma. Lesion is well demarcated from surrounding cancellous bone. Tumor is soft and hemorrhagic, & adjacent cancellous bone is free of tumor. |
TERMINOLOGY
Abbreviations
Plasma cell myeloma (PCM)
Definitions
Plasma cell-based neoplasm composed of a clone of immunoglobulin-secreting, heavy-chain classswitched, terminally differentiated B cells that typically secrete a single homogeneous (monoclonal) immunoglobulin (Ig)
Plasma cell myeloma is a bone-marrow-based, multifocal malignant plasma cell neoplasm associated with M protein in serum &/or urine
Solitary plasmacytoma of bone is a localized malignant bone neoplasm consisting of monoclonal plasma cells
Complete skeletal radiographs show no other lesions
No clinical features of plasma cell myeloma and no evidence of bone marrow plasmacytosis except for solitary lesion
CLINICAL ISSUES
Epidemiology
Incidence
Most common primary malignant bone tumor
Age
Patients usually > 30 years of age at time of diagnosis
Median age at diagnosis: ˜ 70 years
Gender
Males affected more frequently than females
Site
May present as localized lesion (plasmacytoma) or as component of widespread disease (plasma cell myeloma)
May involve any bone
Most common sites are bones with active bone hematopoiesis
In order of frequency: Vertebrae, ribs, skull, pelvis, femur, clavicle, and scapula
Thoracic vertebrae are more commonly involved than cervical or lumbar
Long bone involvement below elbow or knee is rare
Presentation
Pain
Pathologic fracture
Natural History
Plasma cell myeloma
Usually incurable, with survival ranging from 6 months to > 10 years and median survival of 3-4 years
Solitary plasmacytoma
2/3 of patients eventually evolve to generalized myeloma or additional solitary or multiple plasmacytomas
1/3 of patients remain disease free for > 10 years
Treatment
Localized disease treated with resection or radiation
More disseminated disease is incurable, but treatment with combination of chemotherapy and radiation therapy may prolong survival
Bone marrow transplantation is option for younger patients
IMAGE FINDINGS
Radiographic Findings
Geographic lytic lesion centered in bone marrow without identifiable matrix
44% show multiloculated appearance
Lesions in skull are well circumscribed and have punched-out appearance
Lesions of long bones are also usually well circumscribed and may be encompassed by periosteal new bone formation, giving the appearance of expansion
Rarely, myeloma generates sclerotic lesions
May occur in setting of POEMS syndrome
May appear normal or “cold” on isotope scans
MR Findings
T1WI: Low signal intensity soft tissue mass; enhancement with contrast
Fluid-sensitive sequences
Intermediate signal intensity soft tissue lesion
MACROSCOPIC FEATURES
General Features
Friable, soft, and red
Underlying bone is eroded and fragile
MICROSCOPIC PATHOLOGY
Histologic Features
Tumoral mass of plasma cells displacing normal bone marrow elements
Myeloma plasma cells vary from mature forms indistinguishable from normal to immature, plasmablastic, and pleomorphic
Mature plasma cells
Eccentric nucleus with “spoke wheel” or “clockface” chromatin without nucleoli
Basophilic cytoplasm and perinuclear hof
Plasmablasts
Immature forms have more dispersed nuclear chromatin, higher nuclear:cytoplasmic ratio, and, often, prominent nucleoli
Pleomorphic
Nuclear immaturity and pleomorphism rarely occur in reactive plasma cells and are reliable indicators of neoplastic plasma cell myeloma
Cytoplasmic Ig may produce variety of morphologically distinctive findings
Multiple pale bluish-white, grape-like accumulations (Mott cells, Morula cells)
Cherry red refractive round bodies (Russell bodies)
Overstuffed fibrils (Gaucher-like cells)
Crystalline rods; pathognomonic of myeloma
ANCILLARY TESTS
Immunohistochemistry
CD138, CD38 are reliable markers of plasma cells
IHC &/or ISH for light chains shows either kappa- or lambda-light chain-restricted plasma cell population
CD19 is negative
May aberrantly express CD56, CD117, CD20, and CD10
Cytogenetics
Both numerical and structural chromosomal abnormalities are common
Most frequent chromosome translocations involve the heavy chain locus on chromosome 14q32
DIFFERENTIAL DIAGNOSIS
Metastatic Carcinoma and Lymphoma
Poorly differentiated neoplastic cells may mimic other poorly differentiated tumors
Problematic on frozen sections; however, diagnosis can usually be readily made on touch preps
Chronic Osteomyelitis Plasma Cell Infiltration
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


