Aneurysmal Bone Cyst
G. Petur Nielsen, MD
Andrew E. Rosenberg, MD
Key Facts
Terminology
Destructive, expansile benign neoplasm of bone characterized by multiloculated blood-filled cystic spaces
Classified into primary and secondary variants
Clinical Issues
80% develop in 1st and 2nd decades of life
Common sites of involvement
Metaphysis of long bones of upper and lower extremities
Posterior elements of vertebra
Small bones of hands and feet
Present with pain and swelling
Treated with curettage or en bloc resection
Low recurrence rate
Image Findings
May appear aggressive with “blow-out” or marked expansion of bone
Multiloculated and may demonstrate internal soft tissue septa and characteristic fluid-fluid levels
Macroscopic Features
Multiple blood-filled cystic spaces separated by thin, tan-white septa
Microscopic Pathology
Blood-filled cystic spaces
Uniform plump fibroblasts that may be mitotically active
Scattered multinucleated osteoclast-like giant cells
Reactive woven bone that follows contours of cyst walls
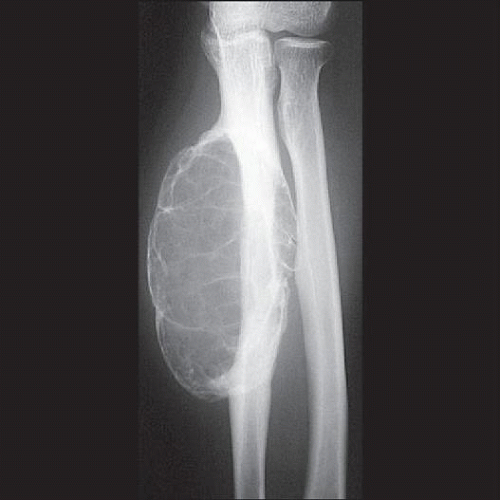 Radiograph shows an eccentric diaphyseal tumor of the ulna extending into the soft tissues that is demarcated by a rim of bone. |
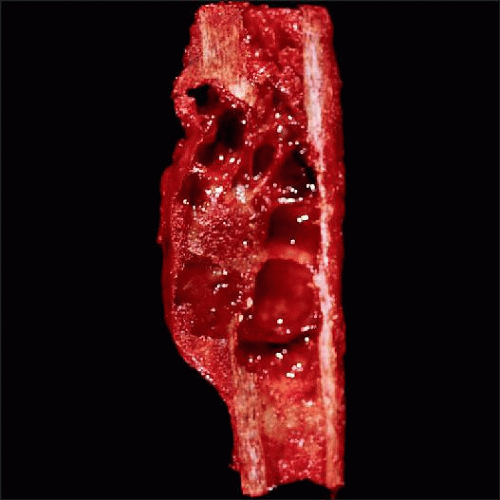 Aneurysmal bone cyst arising in the diaphysis of the fibula consists of hemorrhagic cystic spaces with thin fibrous septae. The cyst has broken through the cortex and extended into adjacent soft tissue. |
TERMINOLOGY
Abbreviations
Aneurysmal bone cyst (ABC) Definitions
Destructive, expansile benign neoplasm of bone characterized by multiloculated, blood-filled cystic spaces
ABCs are classified into primary and secondary variants
ABC, not otherwise specified refers to a primary de novo tumor and accounts for approximately 70% of cases
Secondary ABC is defined as neoplasm that contains areas resembling aneurysmal bone cyst, which arise in background of other types of benign or malignant bone tumors
ETIOLOGY/PATHOGENESIS
Neoplasm
Recent cytogenetic and molecular studies demonstrating t(16;17) strongly suggest that primary ABC is neoplastic
This translocation results in CDH11-USP6 gene fusion transcript
All ABCs with cytogenetic t(16;17) show genomic CDH11 and USP6 rearrangement by FISH
ABCs showing only 17p13 rearrangements show rearrangement of USP6 locus whereas those that show 16q22 rearrangement show rearrangement of CDH11 locus only
CLINICAL ISSUES
Epidemiology
Age
Affects all age groups with most cases (80%) occurring in 1st and 2nd decades of life
Gender
Equal male:female ratio
Site
Metaphysis of long bones of upper and lower extremities
Posterior elements of vertebra
Small bones of hands and feet
Craniofacial skeleton
May also arise in flat bones such as pelvic and scapula bones
Presentation
Pain and swelling
Tumors in spine can cause nerve compression and neurologic symptoms Treatment
Curettage or en block resection Prognosis
Recurrence rate low: Usually recur shortly after treatment (within 6 months)
Spontaneous regression may occur following incomplete removal
Rare reports of apparent malignant transformation of ABC have been described
Unclear whether these tumors represent malignant transformation or ABC-like change in preexisting sarcoma
IMAGE FINDINGS
Radiographic Findings
MR Findings
Multiloculated and may demonstrate internal soft tissue septa and characteristic fluid-fluid levels
Exhibit only modest levels of enhancement
CT Findings
Cystic, expansile, and radiolucent
Bone Scan
Hot on bone scan
MACROSCOPIC FEATURES
General Features
Multiple blood-filled cystic spaces separated by thin, tan-white septa
More solid tan-white areas can also be seen
Either represents a solid portion of ABC wall or primary lesion that has developed secondary ABC-like change
Solid areas within ABC should be thoroughly sampled to identify presence of possible underlying primary neoplasm
MICROSCOPIC PATHOLOGY
Histologic Features
Uniform plump fibroblasts that may be mitotically active
Scattered multinucleated osteoclast-like giant cells
Reactive woven bone
Lined by osteoblasts and follows contours of fibrous septa of cyst walls
Approximately 1/3 of cases contain matrix known as “blue bone”
Infrequently seen in other types of bone tumors
Necrosis uncommon unless there has been a pathologic fracture
Solid ABC lacks blood-filled cystic spaces and is composed of elements that compose cyst wall
May be hypercellular, mitotically active, and contain woven bone
ANCILLARY TESTS
Cytogenetics
Cytogenetic studies have shown t(16;17)
DIFFERENTIAL DIAGNOSIS
Giant Cell Reparative Granuloma
Giant cell reparative granuloma and solid component of ABC are histologically identical
Giant cell reparative granulomas typically arise in small bones and in jaw and do not demonstrate cytogenetic abnormality seen in ABC Telangiectatic Osteosarcoma
Can grossly simulate ABC
Fibrous septa in telangiectatic osteosarcoma contain overtly malignant neoplastic cells with marked pleomorphism and easily identifiable mitotic figures Secondary Aneurysmal Bone Cyst
Variety of benign and malignant bone tumors can develop secondary ABC-like changes
ABCs need to be carefully sampled histologically to exclude any underlying lesion, as tumor will behave as the primary tumor
Secondary ABC does not have cytogenetic abnormalities present in primary ABC
SELECTED REFERENCES
1. Oliveira AM et al: Aneurysmal bone cyst: a neoplasm driven by upregulation of the USP6 oncogene. J Clin Oncol. 24(1):e1; author reply e2, 2006
Image Gallery
Imaging Features
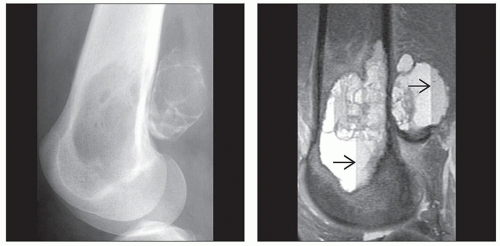 (Left) X-ray of the distal femur shows an aneurysmal bone cyst (ABC) extending into the posterior soft tissues. The intraosseous component is purely lytic and in the soft tissues; it appears mineralized due to the overlying rim of periosteal bone. (Right) T2-weighted MR shows an ABC composed of cystic spaces partitioned by thin membranes. Multiple fluid-fluid levels  represent layering of the cyst components with the heavier (presumably cellular) elements settling to the dependent parts of the lesion. represent layering of the cyst components with the heavier (presumably cellular) elements settling to the dependent parts of the lesion. |
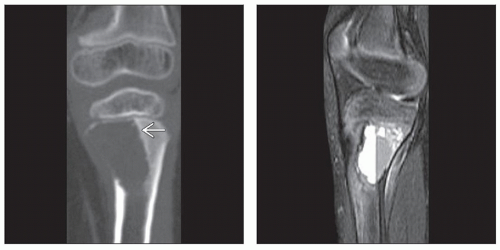
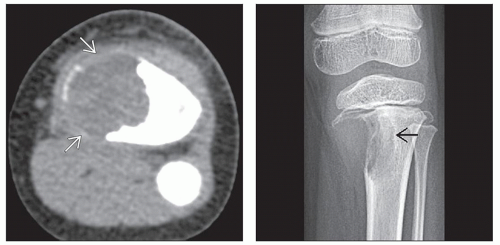 (Left) Axial CT scan through an ABC shows that it has eroded the cortex and is demarcated from the soft tissues by partially mineralized periosteal new bone  . The tumor has mixed signal intensity. (Right) AP radiograph of the knee in a skeletally immature child shows a lytic lesion of the proximal tibial metaphysis extending to the growth plate. The bone margin appears relatively well demarcated and slightly sclerotic . The tumor has mixed signal intensity. (Right) AP radiograph of the knee in a skeletally immature child shows a lytic lesion of the proximal tibial metaphysis extending to the growth plate. The bone margin appears relatively well demarcated and slightly sclerotic  . The soft tissue margin is difficult to identify. . The soft tissue margin is difficult to identify. |
 (Left) Coronal reformatted CT scan shows an ABC that has a sclerotic sharp bony margin  and has eroded the cortex. (Right) T2-weighted MR of an ABC demonstrates a fluid-fluid level that extends across the entire width of the lesion, indicating that there is no solid component. Fluid levels can be seen on CT scans but are best visualized on MR. This may be due to better soft tissue contrast afforded by MR or the fact that an MR examination takes longer to perform, facilitating settling of the cyst contents. and has eroded the cortex. (Right) T2-weighted MR of an ABC demonstrates a fluid-fluid level that extends across the entire width of the lesion, indicating that there is no solid component. Fluid levels can be seen on CT scans but are best visualized on MR. This may be due to better soft tissue contrast afforded by MR or the fact that an MR examination takes longer to perform, facilitating settling of the cyst contents. |
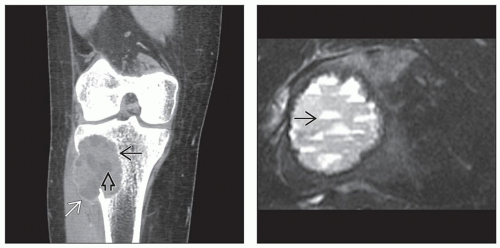 (Left) Reformatted CT scan of an ABC of the tibia shows an eccentric lytic lesion that has a well-formed margin  and a thin shell of periosteal bone and a thin shell of periosteal bone  . Fluid components are identified as low-attenuation areas . Fluid components are identified as low-attenuation areas  , but fluid levels are absent. The patient was supine for this examination, and coronal reformations do not demonstrate fluid levels. (Right) Axial T2-weighted MR of an ABC of the tibia shows multiple fluid levels , but fluid levels are absent. The patient was supine for this examination, and coronal reformations do not demonstrate fluid levels. (Right) Axial T2-weighted MR of an ABC of the tibia shows multiple fluid levels  . The tumor is well circumscribed. . The tumor is well circumscribed. |
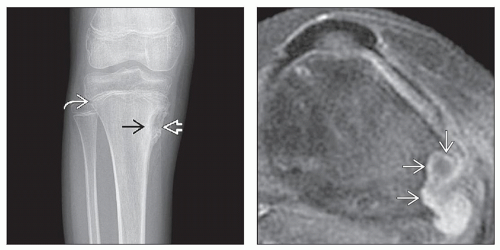 (Left) AP radiograph of a teenager (the growth plate is open
 ) shows an eccentrically located (cortically based) aneurysmal bone cyst of the medial tibia. Laterally, the cyst has a sclerotic rim ) shows an eccentrically located (cortically based) aneurysmal bone cyst of the medial tibia. Laterally, the cyst has a sclerotic rim  whereas medially, it is surrounded by periosteal bone formation whereas medially, it is surrounded by periosteal bone formation  . (Right) Axial T1-weighted, fat-suppressed, contrast-enhanced MR of a cortically based aneurysmal bone cyst shows that the lesion exhibits rim enhancement . (Right) Axial T1-weighted, fat-suppressed, contrast-enhanced MR of a cortically based aneurysmal bone cyst shows that the lesion exhibits rim enhancement  within the cyst walls. within the cyst walls.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|