Enchondroma
G. Petur Nielsen, MD
Andrew E. Rosenberg, MD
Key Facts
Terminology
Common benign primary bone tumor that accounts for approximately 3-10% of all bone tumors
Clinical Issues
Usually presents during 3rd and 4th decades of life
Almost 90% of enchondromas are solitary
Predominate in distal appendicular skeleton
Commonly asymptomatic
Frequently detected as incidental finding
Solitary enchondromas can be followed
Tumors with questionable radiographic findings should be curetted
Image Findings
Spherical or oblong lucent lesion
Well-defined margins
Radiodensities with dense speckled pattern and “arcs and rings”
Macroscopic Features
Range in size from 3-5 cm
Some large enough to produce visible deformities
Pearly white or gray
Nodular architecture with endosteal scalloping
Microscopic Pathology
Composed of cartilaginous nodules
Well circumscribed
Matrix is hyaline
Myxoid matrix is uncommon
Tumors in digits and in setting of Ollier disease and Maffucci syndrome may be more cellular and demonstrate cytologic atypia
 Enchondroma demonstrates classic “ring and arc” pattern corresponding to reactive bone rimming individual cartilage nodules. Spiculated radiodensities represent calcification of the hyaline matrix. |
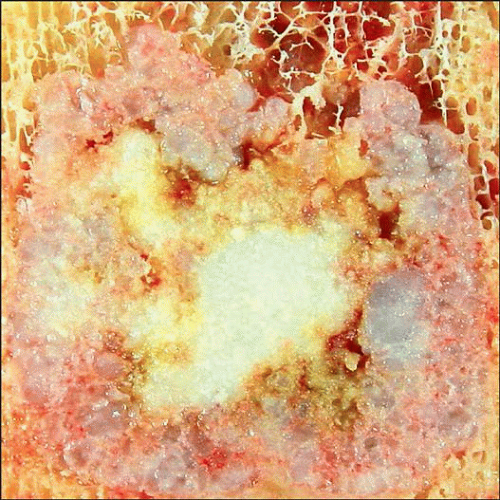 Well-circumscribed enchondroma shows that the tumor is composed of nodules of cartilage that vary in size and are gray-blue and glistening. The tan-white regions represent foci of matrix calcification. |
TERMINOLOGY
Abbreviations
Enchondroma (ench)
Synonyms
Chondroma of bone
Definitions
Benign primary bone tumor composed of chondrocytes producing cartilage matrix that arises within medullary cavity
ETIOLOGY/PATHOGENESIS
Unknown
Likely results from genetic events in stem cells
CLINICAL ISSUES
Epidemiology
Incidence
1 of more common primary bone tumors
2nd in frequency to osteochondroma
Accounts for approximately 12-24% of primary benign bone tumors
Represents 3-10% of all primary bone tumors
Age
Usually presents during 3rd and 4th decades of life
Uncommon in children and elderly
Gender
Equal gender distribution
Ethnicity
No racial predilections
Site
Arise only in bones that form from process of enchondral ossification during embryologic development
Do not develop in bones that are intramembranous in formation
Almost 60% of solitary enchondromas arise in small tubular bones of hands and feet
Represents most common primary bone tumor of hand
Other frequent sites of involvement include long tubular bones (20-45%)
Frequently affected bones are femur, tibia, humerus, fibula
Metaphysis and proximal and distal potions of diaphysis
Uncommon for enchondroma to arise in flat bones and spine
< 3% develop in pelvis
Presentation
Vast majority are asymptomatic
Frequently detected as incidental finding during investigation of other conditions
Relatively common for enchondroma to be diagnosed in patients with pain associated with other abnormalities, such as osteoarthritis, torn menisci, or rotator cuff
Pain is erroneously attributed to enchondroma in periarticular bone
Almost 90% of enchondromas are solitary
Slow growing; may show no growth in adulthood
Infrequently painful except if fractured
Pain caused by generation of microfractures
Painful intraosseous hyaline cartilage tumor should raise possibility of chondrosarcoma
Fractures usually involve phalanges
Large tumors in long bones rarely present with dramatic pathologic fracture
Natural History
Slow limited growth that eventually ceases
Multiple lesions occur in syndromes: Ollier disease, Maffucci syndrome, metachondromatosis
Ollier disease: 2 or more enchondromas
Maffucci syndrome: 2 or more enchondromas associated with superficial soft tissue vascular tumors
Type of vascular tumor in Maffucci syndrome is spindle cell hemangioma
Metachondromatosis: Multiple enchondromas and osteochondromas (autosomal dominant mode of inheritance)
Malignant transformation of isolated lesion into chondrosarcoma very uncommon
Increased incidence of malignant transformation in enchondromatoses
Treatment
Most asymptomatic solitary enchondromas can be clinically followed
Determination of which tumor should be operated upon depends on clinical circumstances
Painful tumors may require therapy to alleviate symptoms and to exclude low-grade chondrosarcoma
Tumors with radiographic findings that raise suspicion of chondrosarcoma should be biopsied or curetted
Some patients may require treatment for psychological reasons
Surgical treatment is usually thorough curettage and packing with bone graft or cement
En bloc resection is performed on sizable lesions in expendable bones, such as proximal fibula or rib
Prognosis
Local recurrence following curettage is uncommon (3-4%)
Local recurrence should raise suspicion of chondrosarcoma
IMAGE FINDINGS
Radiographic Findings
Spherical or oblong in shape
Most tumors are lucent with scattered areas of increased radiodensity
Extent of mineralization varies considerably
Many tumors contain scattered dense stippled opacities
Represent irregular calcification of cartilaginous matrix
Rim of mineralized reactive bone surrounding individual radiolucent nodules of cartilage produce arcs, “O” or “C” ring-like mineralized structures
Progressive mineralization may occur over time and can be mistaken for enlargement of tumor
In older tumors, mineralized nodules coalesce and form solid, stone-like intraosseous density
Focal loss of calcification over time may indicate malignant transformation
Well-defined margins
Margins may or may not be associated with sclerosis
Tumor adjacent to inner cortex produces scalloping
Scalloping has smooth contours
Large tumors in small or flat bones can cause marked thinning of cortex or cortical resorption
Progressively enlarging tumors in small and flat bones can result in significant expansion of bone
Marked asymmetric bone expansion is uncommon and known as enchondroma protuberans
Cortical thinning, bone expansion, and periosteal reaction in combination are usually harbingers of malignancy when associated with cartilage tumors in flat or large tubular bones
Periosteal reaction usually absent unless fracture has occurred
No soft tissue extension or mass
MR Findings
High signal intensity on T2WI
Low to intermediate signal intensity on T1WI
Mineralized cartilage produces signal void
Marrow surrounding tumor is usually normal, except if there has been fracture
Presence of surrounding marrow edema raises possibility of chondrosarcoma
CT Findings
Well-circumscribed lobulated tumor
Stippled calcifications
Arcs, rings, and C-shaped patterns of mineralization
Scalloped endosteum with cortical thinning
No periosteal reaction unless associated with fracture
Bone Scan
May be negative
Actively calcifying tumors show moderate activity
Fractured tumors show marked activity
PET Scan
Enchondroma has SUV of < 2 with 18-FDG PET
MACROSCOPIC FEATURES
General Features
Firm-to-hard; grittiness depends on amount of matrix mineralization and reactive bone formation
Composed of coalescing pearly white or gray nodules that are usually 3-5 mm in diameter
Gray glistening nodules of hyaline cartilage
White areas represent mineralized matrix
Scalloping of endosteal surface may be present
Well demarcated from surrounding bone
Sections to Be Submitted
Process entire tumor in curettage specimen
Resections: Minimum of 1 section per cm
Concentrate on noncalcified regions
Submit closest bone and soft tissue margins
Size
Relatively small; ranges from 1-5 cm
Tumors in small bones may cause deformity of bone
Uncommon for tumor in long bone to be large enough to produce visible distortion
MICROSCOPIC PATHOLOGY
Histologic Features
Composed of variably sized nodules of hyaline cartilage
Fibrocartilage differentiation is rare
Elastic cartilage differentiation extraordinarily rare
Nodules of cartilage well circumscribed and have sharp margin with surrounding bone
Cartilage is hypo- to moderately cellular
Contains chondrocytes that have uniform, small, round, hyperchromatic (lymphocyte-like) nuclei
Occasionally, cells are binucleate and have fine chromatin and small nucleolus
Matrix is usually hyaline type and rarely fibrocartilaginous
Most prominent component of lesion
Myxoid matrix is uncommon
Should raise suspicion for chondrosarcoma
Hyaline matrix frequently calcifies
Calcification appears as amorphous purple or basophilic granular material
Chondrocytes undergo necrosis in zones of calcification
Periphery of nodules often undergoes endochondral ossification
Bone rims nodules of cartilage
No encasement of preexisting trabecular bone (infiltration), which is feature of chondrosarcoma
At periphery of tumor, remnants of cartilage may be in center of broad bony trabeculae
Enchondromas arising in digits are frequently hypercellular and demonstrate mild cytologic atypia
Enchondromas in Ollier disease and Maffucci syndrome may be hypercellular and exhibit cytologic atypia, and matrix may be focally myxoid
ANCILLARY TESTS
Immunohistochemistry
Chondrocytes strongly express vimentin and S100 but do not stain for keratin
Cytogenetics
Abnormalities involving chromosomes 5, 6, 7, 12, and 17
DIFFERENTIAL DIAGNOSIS
Low-Grade Chondrosarcoma
Grows with infiltrative pattern
Greater degree of cellularity
Increased nuclear atypia
Chondromyxoid Fibroma
Contains myxoid and fibrous elements
Lacks well-formed hyaline cartilage
DIAGNOSTIC CHECKLIST
Pathologic Interpretation Pearls
Well-circumscribed tumor composed of nodules of hyaline cartilage
Cartilage hypo- to moderately cellular
Chondrocytes cytologically banal
SELECTED REFERENCES
1. Eefting D et al: Assessment of interobserver variability and histologic parameters to improve reliability in classification and grading of central cartilaginous tumors. Am J Surg Pathol. 33(1):50-7, 2009
2. Romeo S et al: Benign cartilaginous tumors of bone: from morphology to somatic and germ-line genetics. Adv Anat Pathol. 16(5):307-15, 2009
3. Bell WC et al: Molecular pathology of chondroid neoplasms: part 1, benign lesions. Skeletal Radiol. 35(11):805-13, 2006
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


