Fibrosarcoma (Malignant Fibrous Histiocytoma)
G. Petur Nielsen, MD
Andrew E. Rosenberg, MD
Key Facts
Terminology
Malignant fibrous histiocytoma
Collagen-producing fibroblastic and myofibroblastic sarcoma
Clinical Issues
Affects middle-aged and elderly adults
Develops in irradiated bone or in background of Paget disease and bone infarction
Pain
Treated like osteosarcoma of bone
5-year survival rate approximately 60%
Image Findings
Destructive
Poorly circumscribed
Nonmineralized
Microscopic Pathology
High-grade tumor showing fibroblastic and myofibroblastic differentiation
Composed of fascicles of pleomorphic spindle cells frequently arranged in herringbone or storiform pattern
Multinucleated tumor giant cells, necrosis and high mitotic rate often present
Neoplastic cells often embedded within collagen-rich stroma
Ancillary Tests
Immunohistochemical findings in malignant fibrous histiocytoma are nonspecific and generally helpful in excluding other tumors in differential diagnosis
 AP radiograph of the distal femur reveals an eccentric lytic lesion of the metaphysis. It contains small fragments of residual bone engulfed by the tumor (sequestra). The margins are “moth-eaten.” |
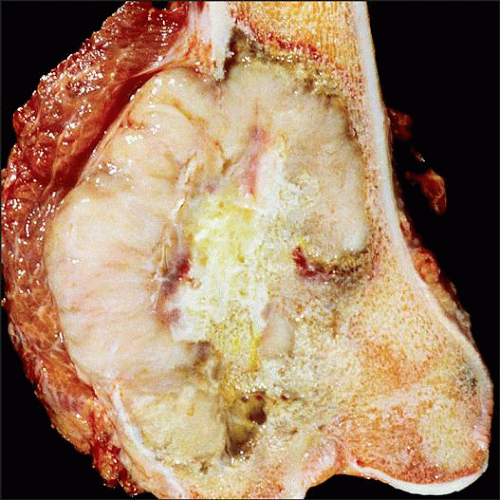 Fibrosarcoma of the distal femur appears as a variegated tan fleshy mass with pale yellow areas of necrosis and foci of hemorrhage. The tumor destroys the cortex and extends into the soft tissues. |
TERMINOLOGY
Abbreviations
Fibrosarcoma (FSA)
Synonyms
Pleomorphic malignant fibrous histiocytoma
Undifferentiated pleomorphic sarcoma
Fibroxanthosarcoma
Malignant fibrous xanthoma
Definitions
High-grade sarcoma showing fibroblastic &/or myofibroblastic differentiation
ETIOLOGY/PATHOGENESIS
Neoplastic
In most tumors, there is no known predisposing factor
Approximately 20% of malignant fibrous histiocytomas arise in preexisting condition (secondary fibrosarcoma)
Paget disease
Patients with history of radiation to bone
Bone infarct
Diaphyseal medullary stenosis
Can also arise in association with prosthetic devices
CLINICAL ISSUES
Epidemiology
Incidence
Rare tumor
Approximately 2% of primary malignant bone tumors
Age
Wide age group but usually affects middle-aged and elderly individuals
Most patients are > 50 years old at time of diagnosis
Rare cases occur in young individuals
Site
Long bones
Most commonly femur followed by tibia and pelvis
Usually arises in metaphysis or diaphysis of long bones
Presentation
Pain
Mass
Pathologic fracture
Treatment
Treated like osteosarcoma of bone
Combination of chemotherapy and surgery ± radiation therapy
Prognosis
5-year survival rate approximately 40-50%
Lung most common site for distant metastases
IMAGE FINDINGS
Radiographic Findings
Radiographic features are nonspecific and indicate an aggressive malignant neoplasm
Destructive
Lytic mass with “moth-eaten” pattern of destruction
Small sequestered fragments of residual bone may be present
Poorly circumscribed
Generally no sclerotic margin
If present, it is incomplete
Metaphyseal and usually eccentrically located
Cortical breakthrough and soft tissue mass commonplace
May be signs of preexisting lesion
MR Findings
CT Findings
Similar to radiographic findings
Bone Scan
Hot on bone scan
MACROSCOPIC FEATURES
General Features
Variable gross appearance
Can be tan-white with areas of hemorrhage and necrosis
Involving medullary cavity and extending into adjacent soft tissue
Size
Usually large at time of diagnosis
MICROSCOPIC PATHOLOGY
Histologic Features
Identical to soft tissue counterpart
Very diverse morphologic features with different patterns
Most common subtypes in bone are storiform pleomorphic type and giant cell-rich type
Fascicles of pleomorphic spindle-shaped cells arranged in a fascicular or storiform/pinwheel growth pattern
Multinucleated osteoclast-type giant cells are present in giant cell-rich type
Necrosis and a high mitotic rate, including presence of atypical mitotic figures, is common
Neoplastic cells often embedded within collagen-rich stroma that may be hyalinized
Often difficult to differentiate hyalinized collagen stroma from osteoid
Cells with epithelioid morphology, prominent vasculature with hemangiopericytoma-like growth pattern may also be present
Myxoid change commonly seen in myxofibrosarcoma of soft tissue, which is much less frequently encountered among intraosseous tumors
Rare cases of sclerosing epithelioid fibrosarcoma have been reported
ANCILLARY TESTS
Immunohistochemistry
Immunohistochemical findings in malignant fibrous histiocytoma are nonspecific and generally helpful in excluding other tumors in differential diagnosis
Neoplastic cells are diffusely positive for vimentin and may show focal staining for smooth muscle markers
Indicative of fibroblastic and myofibroblastic differentiation
Occasionally, tumor cells may show some keratin positivity, raising possibility of metastatic sarcomatoid carcinoma
Neoplastic cells can also stain for histiocytic markers
Electron Microscopy
Ultrastructurally, neoplastic cells usually show fibroblastic differentiation containing abundant intracytoplasmic rough endoplasmic reticulum
Some cells may contain myofibroblastic differentiation with peripheral filaments and densities
Some cells contain intracytoplasmic lysosomes (fibrohistiocytes)
DIFFERENTIAL DIAGNOSIS
High-Grade Osteosarcoma
Presence of extracellular collagen deposition in fibrosarcoma can sometimes be difficult to differentiate from neoplastic bone
Any mineralization of collagen fibers is suggestive of bone formation
Sometimes diagnosis of osteosarcoma does not become apparent until after resection when neoplastic bone is appreciated
Fortunately, both high-grade fibrosarcoma of bone and osteosarcoma are treated with osteosarcoma protocol and show similar response to chemotherapy
Dedifferentiated Chondrosarcoma
Dedifferentiated component in dedifferentiated chondrosarcoma is usually composed of undifferentiated pleomorphic sarcoma
Radiographic correlation is helpful in identifying underlying low-grade cartilaginous tumor
Metastatic Sarcomatoid Carcinoma
When high-grade fibrosarcoma is keratin positive, metastatic sarcomatoid carcinoma has to be excluded
Presence of single bone lesion favors primary bone tumor
In some cases, electron microscopy can be helpful
Leiomyosarcoma
High-grade leiomyosarcoma can have similar histologic features
Neoplastic cells in leiomyosarcoma usually have more abundant eosinophilic cytoplasm
Stain for muscle markers such as desmin, muscle actin, and smooth muscle actin
Ultrastructurally, they show smooth muscle differentiation
Malignant Lymphoma
Can mimic fibrosarcoma radiographically
Easy to differentiate by light microscopy
Angiosarcoma
Usually lytic and highly aggressive radiographically
Easy to distinguish histologically
Angiosarcoma stains for endothelial markers, which are negative in fibrosarcoma
DIAGNOSTIC CHECKLIST
Pathologic Interpretation Pearls
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


