Penile Intraepithelial Neoplasia (PeIN)
Elsa F. Velazquez, MD
Antonio L. Cubilla, MD
Key Facts
Terminology
Most warty/basaloid PeIN replace most or entire thickness of epithelium and represent carcinoma in situ
Low-grade warty/basaloid PeIN (atypical cells replacing only lower part of epithelium) is exceptional
Differentiated (simplex) PeIN is considered a high-grade lesion
Microscopic Pathology
Differentiated (simplex) PeIN
Elongated and anastomosing rete ridges
Atypical basal cells with hyperchromatic nuclei
Subtle abnormal maturation (large eosinophilic keratinocytes)
Whorling and keratin pearl formation
Usually associated with lichen sclerosus
Basaloid PeIN
Basaloid cells replace most to full thickness of epithelium
Prominent apoptosis and mitosis
Warty PeIN
Pleomorphic cells with koilocytic changes replace most to full thickness of epithelium
Undulated/spiky surface
Warty-basaloid PeIN
Pleomorphic cells with koilocytic changes seen on upper epidermis
Basaloid cells replace lower epidermis
Usually undulated/spiky surface
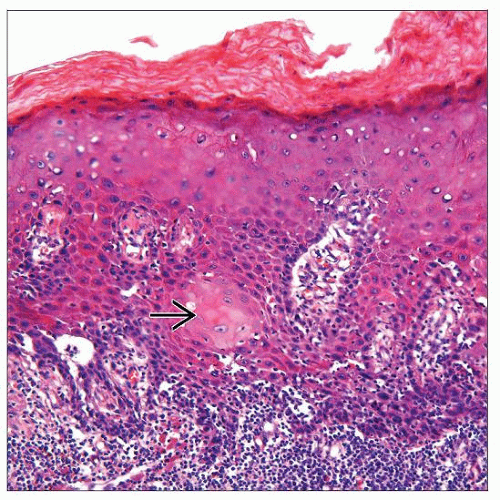 Note the enlarged keratinocytes with abundant eosinophilic cytoplasm throughout most of the epithelium in differentiated PeIN. Characteristic keratin pearl formation is present  . . |
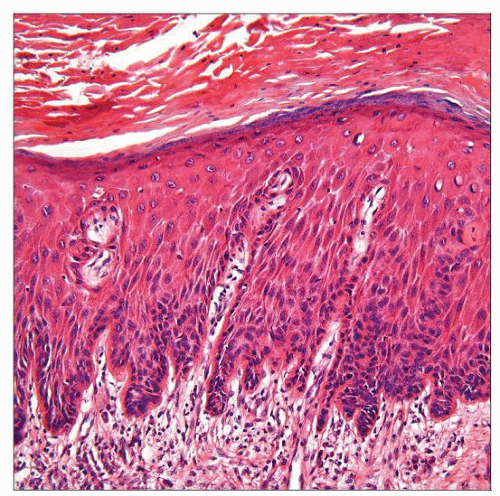 Acanthotic epithelium with subtle abnormal maturation and hyperchromatic atypical basilar cells are features of differentiated PeIN. Parakeratosis is seen on the surface. |
TERMINOLOGY
Abbreviations
Penile intraepithelial neoplasia (PeIN)
Synonyms
Erythroplasia of Queyrat, Bowen disease, squamous cell carcinoma in situ, squamous intraepithelial lesion (SIL)
Definitions
PeIN is considered intraepithelial (in situ) precursor lesion of invasive SCC
ETIOLOGY/PATHOGENESIS
Pathogenesis
Basaloid, warty and warty/basaloid (undifferentiated) PeIN are HPV-related (especially HPV-16)
Differentiated (simplex) PeIN is unrelated to HPV
Lichen sclerosus may be implicated in pathogenesis of differentiated PeIN
CLINICAL ISSUES
Epidemiology
Incidence
Real incidence is unknown
2/3 associated with invasive SCC
When invasive SCC is associated with PeIN, 65% are differentiated PeIN and 35% are undifferentiated PeIN
Age
5th and 6th decades
Presentation
Differentiated PeIN
Seen in older patients, frequently affects foreskin
Usually arises in setting of chronic scarring, inflammatory dermatosis, especially lichen sclerosus
Warty/basaloid PeIN
Seen in younger patients; usually affects glans, perimeatal region
Usually not associated with lichen sclerosus
Patients may have history of condyloma
Treatment
Surgery, locally destructive treatments
Prognosis
Since most studies on PeIN are retrospective analyses of lesions associated with invasive SCCs, real prognosis of PeIN remains unknown
MACROSCOPIC FEATURES
General Features
Gross appearance of PeIN is heterogeneous
Gross appearance does not allow distinction between different types
Uni- or multifocal
Sharp or ill-defined borders
Flat to slightly elevated hyperkeratotic or even papillary lesions
Pearly white, moist, erythematous, dark brown/black
Macules, papules, or plaques
Differentiated PeIN usually arises in background of lichen sclerosus
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


