• High grade: Marked nuclear atypia, loss of polarity, cribriforming, luminal necrosis
Top Differential Diagnoses
• Intraductal papillary mucinous neoplasm
• Reactive ductal epithelial changes
• Intraductal spread of invasive carcinoma (cancerization of ducts)
Diagnostic Checklist
• High-grade PanIN should be noted in pathology reports, especially in absence of invasive carcinoma
• Low-grade PanIN does not need to be reported, does not affect surgical management
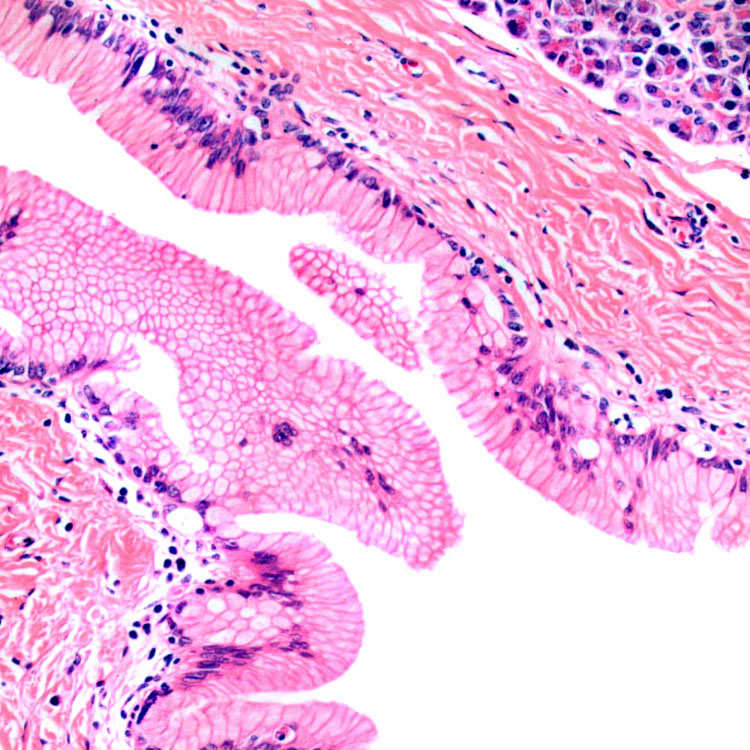
Low Grade (PanIN-1) Pancreatic duct lined by a single layer of epithelium is shown with abundant apical mucinous cytoplasm and basal nuclei that lack atypia [formerly pancreatic intraepithelial neoplasia (PanIN)-1a].
Low Grade (PanIN-2) The lining cells show enlarged hyperchromatic nuclei and a slight loss of nuclear polarity . The cytologic atypia distinguishes it from PanIN-1. Both PanIN-1 and PanIN-2 are now classified as low-grade PanIN.
Low-grade PanIN, Micropapillary Pattern Pancreatic duct lined by a micropapillary proliferation of mucinous epithelial cells . There is nuclear crowding and hyperchromasia indicating low-grade PanIN. This was formerly referred to as PanIN-2.
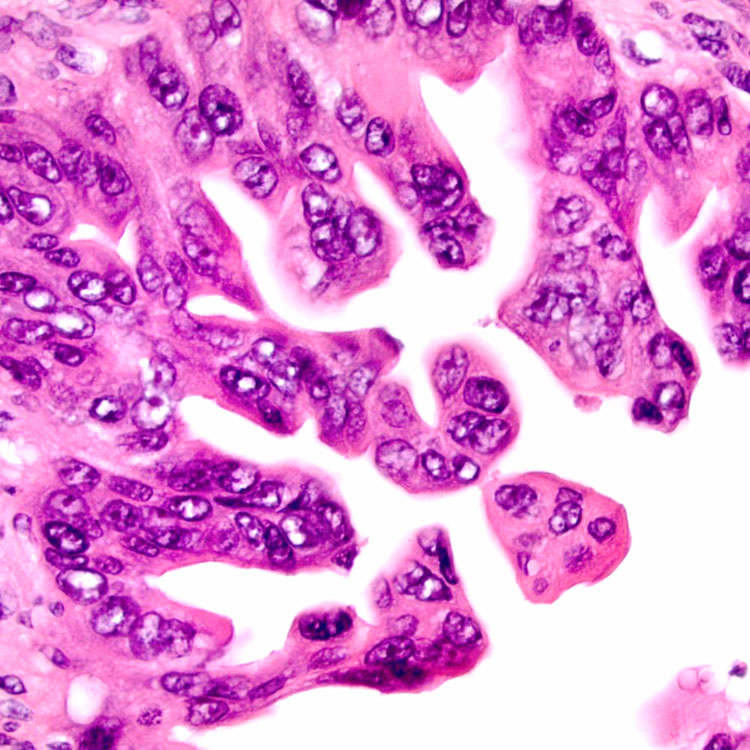
High-Grade PanIN The pancreatic duct is lined by epithelial cells with micropapillary architecture, prominent cytologic atypia, variably prominent nucleoli, and loss of polarity (formerly referred to as PanIN-3).

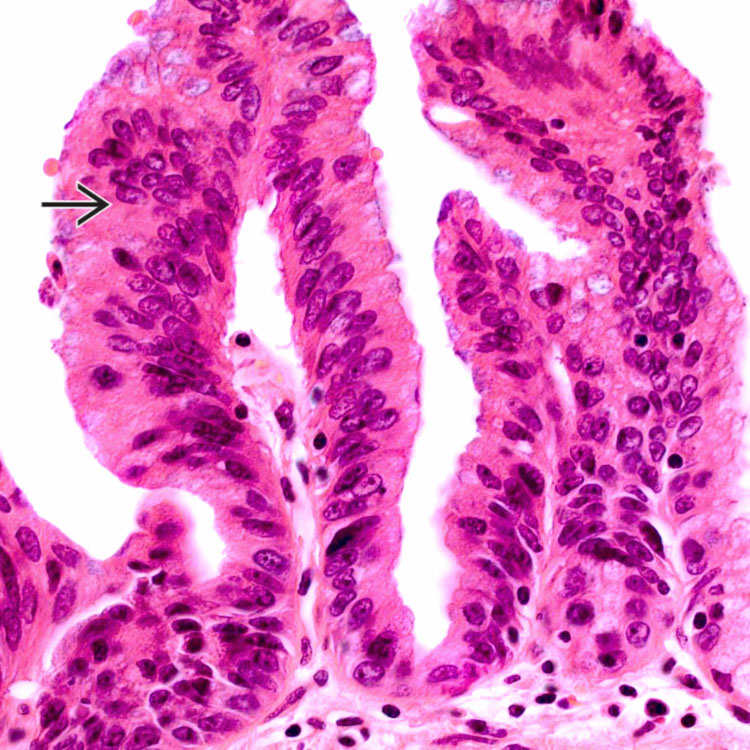
 . The cytologic atypia distinguishes it from PanIN-1. Both PanIN-1 and PanIN-2 are now classified as low-grade PanIN.
. The cytologic atypia distinguishes it from PanIN-1. Both PanIN-1 and PanIN-2 are now classified as low-grade PanIN.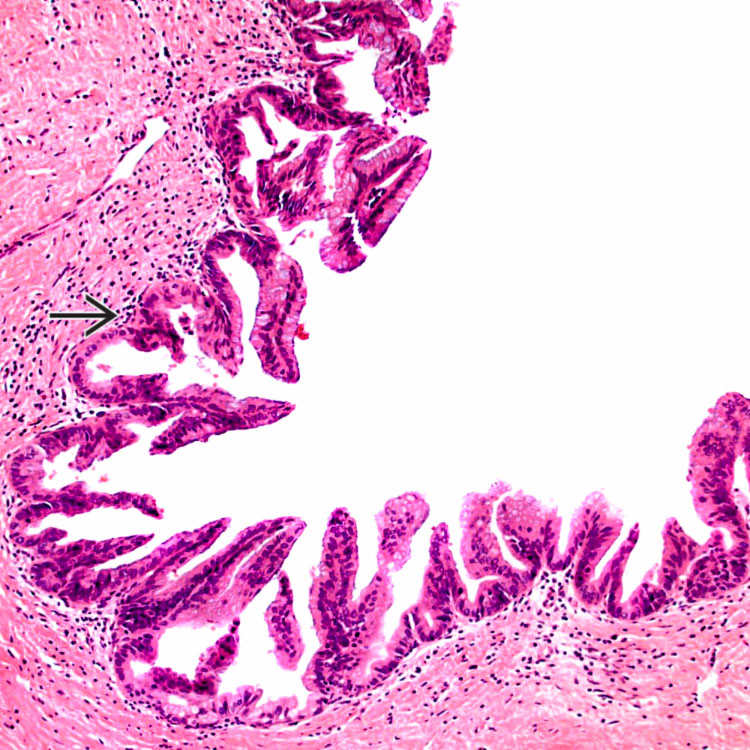
 . There is nuclear crowding and hyperchromasia indicating low-grade PanIN. This was formerly referred to as PanIN-2.
. There is nuclear crowding and hyperchromasia indicating low-grade PanIN. This was formerly referred to as PanIN-2.