http://evolve.elsevier.com/McCuistion/pharmacology
Nutrients are substances that nourish and aid in the development of the body. Nutrients provide energy, promote growth and development, and regulate body processes. Inadequate nutrient intake can cause malnutrition. Patients experiencing chronic or critical illnesses that result in surgery or hospitalization are at risk for malnutrition. Without adequate nutritional support, the body’s metabolic processes slow down or stop. This can greatly diminish organ functioning and have a poor response on the patient’s immune system.
The length of time a person may survive without nutrients is influenced by body weight and composition, genetics, health, and hydration. Patients who are critically ill may only tolerate a lack of nutrient support for a short period before organ failure occurs. Recovery is more rapid for patients who have experienced trauma, burns, or critical illness if nutrition is started within 24 to 48 hours of admission. Administration of enteral nutrition early on restores intestinal motility, maintains gastrointestinal (GI) function, reduces the movement of bacteria and other organisms, improves wound healing, decreases the incidence of infection, and ultimately decreases the length of the hospital stay. Early nutritional support improves the patient’s general health and produces favorable outcomes.
In addition to nutrients, both hydration and electrolyte balance must be considered. If all three are not addressed, preventable complications like constipation, urinary tract infection, and pressure ulcers can occur. The requirements for fluid balance are usually between 30 and 35 mL/kg/day. A healthy person requires 2000 calories per day; critically ill patients require 50% more than the normal energy requirement (approximately 3000 calories per day). If a patient has a 10% weight loss within the last 3 to 6 months and has had little or no nutrition for more than 5 days, nutritional supplementation should be considered. Nutrition and hydration are essential components necessary for everyday life.
Different Types of Nutritional Support
Oral Feeding
Many patients require nutritional supplementation due to malnutrition or anorexia (e.g., a deficiency of certain nutrients, vitamins, or minerals). Many factors can affect appetite: psychological stress about a patient’s illness and problems with family, finances, and employment are just a few of the many challenges a patient may experience. If the patient can swallow and has a working GI tract, oral nutritional supplementation between meals can help increase caloric intake. Many commercially available products can be used to supplement intake. These are marketed as puddings, bars, and supplemental nutritional drinks.
Enteral Nutrition
Enteral nutrition (EN) involves the delivery of nutrition or fluid via a tube into the GI tract, which requires a functional, accessible GI tract. Depending on the different pathologies present, EN may be used for short-term nutritional supplementation, such as with reduced appetite or swallowing difficulties, or long-term nutritional supplementation for malabsorption disorders or increased catabolism.
Routes for Enteral Feedings
A multidisciplinary team approach is used when a decision is required in regard to which feeding route to use. Many factors are considered: the patient’s condition, preferences, the length of the feeding, physiologic conditions, tolerance, and the integrity of the patient’s GI tract.
The gastrointestinal routes used for enteral tube feedings are the nasogastric, nasoduodenal/nasojejunal, gastrostomy or jejunostomy routes (Fig. 14.1). The nasogastric and gastrostomy routes deliver food directly to the stomach. The nasoduodenal/nasojejunal and the jejunostomy routes deliver food after the stomach or below the pyloric sphincter and are used for patients at risk for aspiration. These gastrointestinal routes deliver food by a tube inserted through the nose (nasogastric, nasoduodenal/nasojejunal) or directly into the GI tract (gastrostomy or jejunostomy) through the abdominal wall. The nasogastric, nasoduodenal, and nasojejunal routes are for short-term nutrition of less than 4 weeks’ duration. If long-term nutrition is required, the patient may receive a gastrostomy or a jejunostomy tube placed in the stomach or small bowel by a surgical, endoscopic, or fluoroscopic procedure.
The gastrointestinal tubes are small in diameter, are made of urethane or silicone, and are flexible and long. They are radiopaque, which makes their position easy to identify by x-ray. These tubes easily clog, especially when using thick feedings and when the patient’s medications are crushed and put down the tube. Always flush the tube before and after medication administration and when determining residual volume, so the tube remains patent and does not clog. If the tube becomes clogged, a new tube may have to be placed, which results in extra discomfort to the patient. It is important to note that these tubes can become dislodged, knotted, or kinked during patient coughing or vomiting. The gastrostomy tube, also known as the percutaneous endoscopic gastrostomy (PEG) tube and the jejunostomy (J) tube are placed surgically, endoscopically, or radiologically. With the PEG tube, the patient must have an intact GI system. For patients with chronic reflux, a J-tube is placed either endoscopically or with laparoscopic surgery. Usually, the doctor orders intravenous (IV) antibiotics to decrease the risk of infection. After placement, always check your facility’s policy prior to initiating the tube feeding and use correct nursing procedure when putting medication and food through the tubes. Before the initial feeding, the policy in most facilities is to confirm correct placement of the tube with an x-ray.
Enteral Solutions
Many different types of enteral formulas are used for enteral feedings. These solutions differ according to their various nutrients, caloric values, and osmolality. The four groups of enteral solutions are (1) polymeric (milk-based, blenderized foods and commercially prepared whole nutrient formulas); (2) modular formulas (protein, glucose, polymers, and lipids); (3) elemental/monomeric formulas (predigested nutrients that are easier to absorb); and (4) specialty formulas designed to meet specific nutritional needs in certain illnesses such as liver failure, pulmonary disease, or HIV infection (Table 14.1). Some of the components of enteral solutions include (1) carbohydrates in the form of dextrose, sucrose, lactose, starch, or dextrin (the first three are simple sugars that are absorbed quickly); (2) protein in the form of intact or hydrolyzed proteins or free amino acids; and (3) fat in the form of corn, soybean, or safflower oil (some have a higher oil content than others). With all EN, sufficient water is needed to maintain hydration.
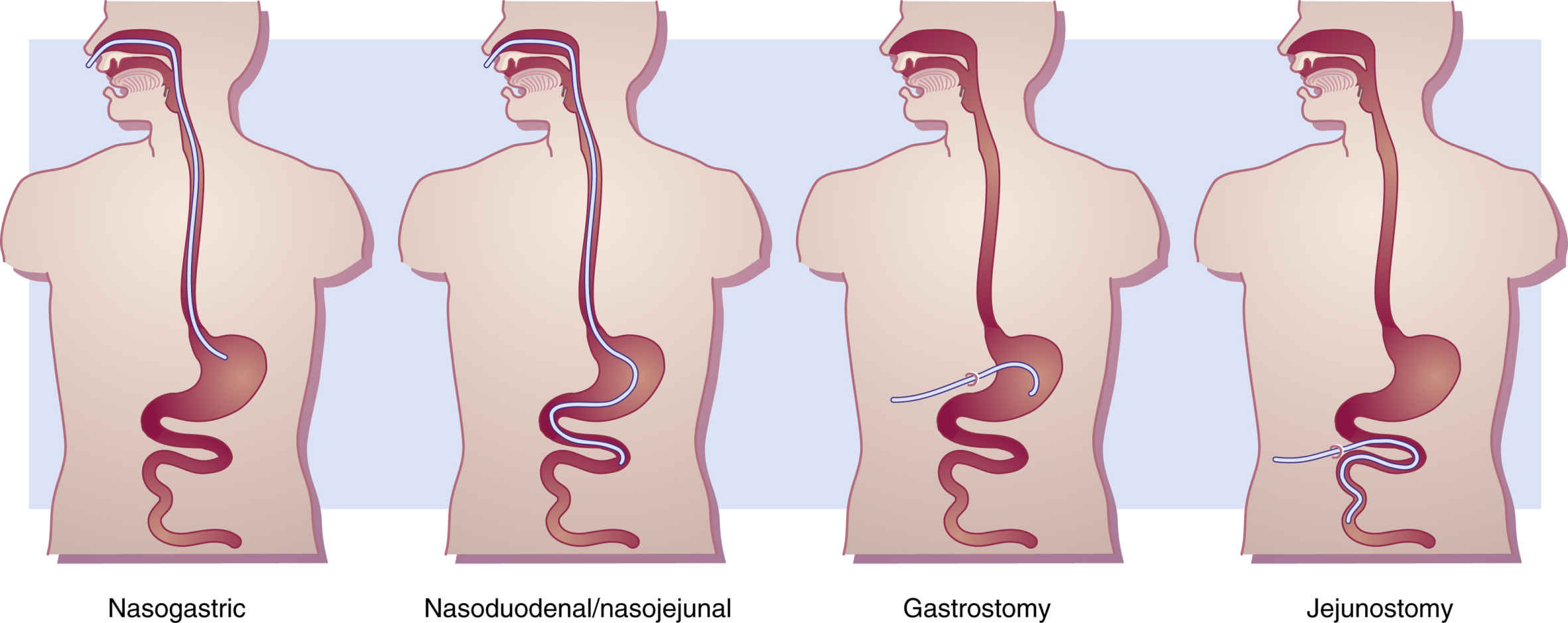
FIG. 14.1 Types of Gastrointestinal Tubes Used for Enteral Feedings.
A nasogastric tube is passed from the nose into the stomach. A weighted nasoduodenal/nasojejunal tube is passed through the nose into the duodenum/jejunum. A gastrostomy tube is introduced through a temporary or permanent opening on the abdominal wall (stoma) into the stomach. A jejunostomy tube is passed through a stoma directly into the jejunum.
Methods for Delivery
Enteral feedings are given by continuous infusion pump, intermittent infusion by gravity, intermittent bolus by syringe, and cyclic feedings by infusion pump. Continuous feedings are prescribed for the critically ill and for those who receive feedings into the small intestine. The enteral feedings are given by an infusion pump such as the Kangaroo pump, which is set to control the flow at a slow rate over 24 hours. Intermittent enteral feedings are administered every 3 to 6 hours over 30 to 60 minutes by gravity drip or infusion pump. At each feeding, 300 to 400 mL of solution is administered. Intermittent infusion is considered an inexpensive method for administering EN. The bolus method was the first method used to deliver enteral feedings, and with this method, 250 to 400 mL of solution is rapidly administered through a syringe into the tube four to six times a day. This method takes about 15 minutes each feeding, but it may not be tolerated well by the patient because a massive volume of solution is given in a short period. The bolus method may cause nausea, vomiting, aspiration, abdominal cramping, and diarrhea; a healthy patient can normally tolerate the rapidly infused solution, therefore this method is reserved for ambulatory patients. The cyclic method is another type of continuous feeding infused over 8 to 16 hours daily (day or night). Administration during daytime hours is suggested for patients who are restless or for those who have a greater risk for aspiration. The nighttime schedule allows more freedom during the day for patients who are ambulatory.
Complications
Dehydration can occur in patients receiving enteral nutrition. Diarrhea is a common complication that can lead to dehydration. High-protein formulas can also cause dehydration, and hyperosmolar solutions can draw water out of the cells in an attempt to maintain serum isoosmolality. Fluid intake is monitored, and if appropriate, fluid is added to the patient’s daily regimen of feedings. Unless contraindicated, it is recommended that 30 to 35 mL/kg/day be maintained for fluid balance in most patients.
Aspiration pneumonitis is one of the most serious and potentially life-threatening complications of tube feedings. It can occur when the contents of the tube feeding enter the patient’s lungs from the GI tract. Consequences range from coughing and wheezing to infection, tissue necrosis, and respiratory failure. An important nursing intervention is to check the agency’s policy for specific guidelines prior to initiating EN. It is imperative that the nurse check for gastric residual by gently aspirating the stomach contents before initiating enteral feeding and thereafter every 4 hours between feedings. Usually, if the residual is greater than 150 mL (check the agency policy), the nurse holds the feeding, and the residual is checked again in 1 hour. If the residual still exceeds this amount, the provider is notified. Large residuals mean the patient may have an obstruction or a problem that is important to correct prior to continuing the feeding.
Another common problem of enteral feeding is diarrhea. Rapid administration of feedings, contamination of the formula, low-fiber formulas, tube movement, and various drugs can all cause diarrhea. Check for drugs that can cause diarrhea; these may be antibiotics or sorbitol in liquid medications. Diarrhea can usually be managed or corrected by decreasing the rate of infusion, diluting the solution with water, changing the solution, discontinuing the drug, increasing the patient’s daily water intake, or administering an enteral solution that contains fiber. Constipation is another common problem that frequently occurs. It can be easily corrected by changing the formula, increasing water, or requesting a laxative.
Patients who have a long history of poor caloric intake are at risk for refeeding syndrome, which describes a cascade of metabolic and electrolyte imbalances that occur as a result of feeding a patient who is nutritionally starved for a prolonged period. Long-term undernutrition causes loss of electrolytes, vitamins, and minerals; this affects biologic processes and organ systems and can lead to abnormally low serum levels of potassium, phosphate, and magnesium that can result in cardiac arrhythmias, respiratory distress, and death. When a malnourished patient is overfed, physiologic burdens occur that put demands on cellular function and body organs. Prevention of refeeding syndrome involves ensuring that feeding begins slowly, at calorie levels below maintenance needs, and is gradually advanced.
Monitoring is essential when the patient is receiving EN. Recommended parameters to monitor include blood chemistry, blood urea nitrogen (BUN), creatinine, and electrolytes; glucose; triglycerides; serum proteins; intake and output; and weight. Frequency of monitoring is patient dependent and should be implemented during the entire EN process.
Enteral Safety
The nurse has an important role in administering tube feedings safely. Some of the important safety concerns are patient position, aspiration risk, residual volumes, and tube position. The head of the bed should be elevated to 30 to 45 degrees during the feeding, and if intermittent, keep the head of the bed elevated for 30 to 60 minutes after the feeding. By elevating the head of the bed, the risk of aspiration is decreased. Ensure the patient has audible bowel sounds by performing a GI assessment with auscultation. This ensures a working GI tract. Always check the gastric residual volume prior to initiating tube feedings and every 4 to 6 hours if the feedings are continuous. Always confirm the position of newly inserted tubing before beginning the first feeding. Initially, after the tube is placed, most agencies require an x-ray to confirm placement. Always follow the agency’s policy and procedure for initial confirmation of placement. Prior to each enteral feeding, placement should be confirmed to ensure the tubing has not moved and is still in the GI tract. Some agencies require pH testing of gastric secretions, whereas others recommend listening for gurgling sounds after inserting air into the tubing. Each of these measures has limitations, so more than one bedside test may be used for confirmation. Always check the agency guidelines. Electromagnetic tracking devices are being associated with reduced tube misplacement, although this technique is still new and is not available to everyone.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


