8 Nervous system
ANATOMY
CRANIAL CAVITY
The cranial cavity has a cranial vault and the base of the cranium with the three cranial fossae.
Cranial vault
The cranial vault, or the roof of the cranial cavity, is formed by the frontal bone anteriorly, the paired parietal bones laterally and the occipital bone posteriorly (Fig. 8.1). In about 8% of cases a metopic suture pre-sents in the midline during early stages of development between the two halves of the frontal bones and persists in adulthood. A midline sagittal groove marks the position of the superior sagittal sinus. The sinus and its groove widen as they pass posteriorly. The falx cerebri is attached to the lips of this groove. Irregular depressions along the groove lodge the arachnoid granulations.
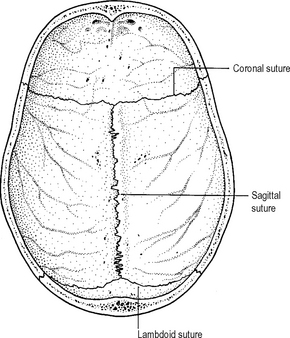
Fig. 8.1 The vault of the skull from below.
Source: Rogers A W, Textbook of anatomy; Churchill Livingstone, Edinburgh (1992)
The lambda is the junction between the lambdoid suture and the sagittal suture. It is the area of the posterior fontanelle in the infant. The bregma, where the anterior fontanelle was in the infant, is at the junction between the coronal and the sagittal sutures. The glabella is the prominence above the nasion which is the depression between the two supraorbital margins. The pterion is a thin part of the skull at the junction of the parietal, frontal and temporal bones and the greater wing of the sphenoid in the temporal region of the skull. The anterior branch of the middle meningeal artery and the accompanying vein traverse the pterion.
Three cranial fossae
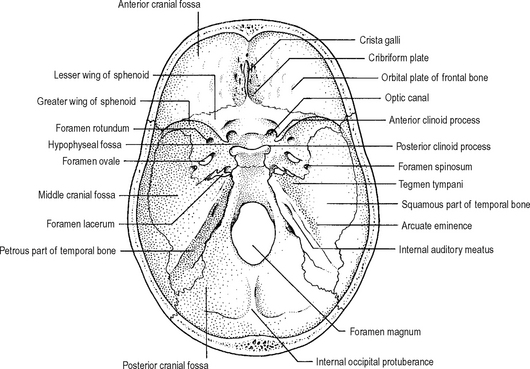
Anterior cranial fossa
The anterior cranial fossa (Fig. 8.2) is largely formed by the orbital plate of the frontal bone supplemented posteriorly by the lesser wing of the sphenoid. The ethmoid bone with its cribriform plate and the crista galli occupies the gap between the two orbital plates. The orbital plate separates the anterior cranial fossa from the orbit. The cribiform plate roofs the nasal cavities.
The following structures pass between the anterior cranial fossa and the nasal cavities.
A fracture of the anterior cranial fossa may cause bleeding into the nose and/or orbit and CSF rhinorrhea. Bleeding into the orbit may manifest as subconjunctival haemorrhage and/or proptosis.
Middle cranial fossa
The body of the sphenoid lies in the middle forming the floor of the pituitary (hypophyseal) fossa (Fig. 8.2). Laterally are the greater wings of the sphenoid and the squamous parts of the temporal bones. The petrous part of the temporal bone containing the middle and inner ear forms the posterior boundary of the fossa.
Lateral to the pituitary fossa the middle cranial fossa has a few important foramina:
BRAIN AND MENINGES
Brain
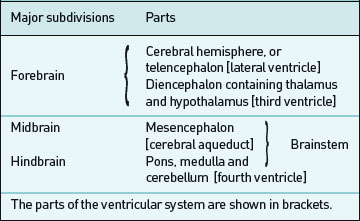
The brain is subdivided into the forebrain, midbrain and hindbrain, comprising the major parts listed in Table 8.1.
Table 8.1 Major subdivisions and parts of the brain
Cerebral hemisphere
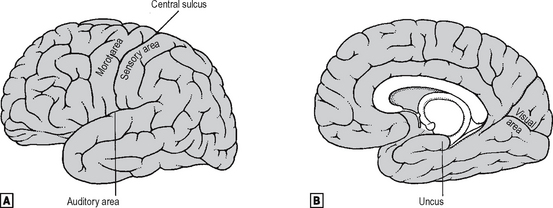
The cerebral hemisphere (Fig. 8.3) is divided into four lobes for descriptive purposes:

The cerebral cortex has a large number of sulci (clefts) and gyri (folds). The lateral sulcus is the largest sulcus on the superolateral surface and separates the temporal lobe from the parietal and frontal lobes (Fig. 8.3).
Major functional areas of the cortex
A number of major functional areas are located in the various lobes of the cerebral hemisphere (Fig. 8.4).
 lateral view.
lateral view.  medial view.
medial view.The olfactory impulses are linked with the temporal lobe in the region of the uncus. The auditory cortex lies on the superior temporal gyrus on the lateral surface of the hemisphere. The visual pathways reach the occipital cortex around the calcarine sulcus. The major motor area of the cortex is the precentral gyrus, from which fibres pass through the internal capsule to the motor nuclei of the cranial and spinal nerves. The somatic sensory cortex, which is mostly the postcentral gyrus, receives afferents from the thalamus carrying various sensory modalities. The motor elements of speech are centred on the Broca’s area in the posterior part of the inferior frontal gyrus of the dominant hemisphere. Both pre- and postcentral gyri have somatotopic representation as shown in the homunculus in Fig. 8.5.

Clinical problems associated with lesions of the various cortical areas
Basal ganglia
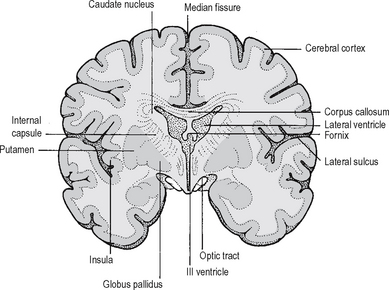
These nuclei are situated deep in the cerebral hemisphere and consist of the corpus striatum – containing the caudate nucleus, the putamen and the globus pallidus (Fig. 8.6) – and the claustrum and the amygdala. The putamen and the globus pallidus are together known as the lentiform nucleus. The lentiform nucleus is separated from the thalamus and the caudate nucleus by the internal capsule. The caudate nucleus and the putamen receive their afferent fibres mostly from the cerebral cortex and the thalamus and send their efferents to the globus pallidus. Efferents from the globus pallidus go to the thalamus, substantia nigra, red nucleus and the reticular formation in the brainstem. The basal ganglia and their connections form the major part of the extrapyramidal system.
The diencephalon is the middle portion of the forebrain. It consists of the thalamus, the hypothalamus and the third ventricle. A faint groove running from the interventricular foramen to the cerebral aqueduct separates the thalamus from the hypothalamus. The thalamus is the major relay centre in the sensory pathway. Most sensations are carried from lower levels through various sensory tracts to the thalamic nuclei, from wherethey are relayed to the sensory cortex. The hypothalamus, lying antero-inferior to the thalamus, is the coordinating area for visceral functions; it also contains centres for endocrine functions.
Hindbrain
The hindbrain (Fig. 8.7) lies below the tentorium cerebelli in the posterior cranial fossa. Its brainstem components, the pons and the medulla, lie on the clivus and extend from the midbrain downwards where it passes through the foramen magnum to become continuous with the spinal cord. The cerebellum projects posteriorly, occupying most of the posterior cranial fossa. The fourth ventricle, which is the cavity of the hindbrain, lies between the brainstem and the cerebellum.
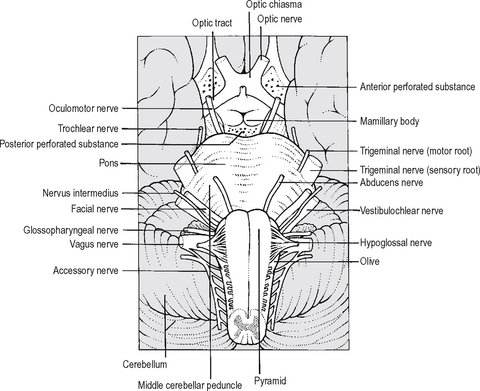
The anterior part of the pons contains fibres largely composed of those descending from the higher centres to synapse in the pontine nuclei. These fibres are relayed to the cerebellum as the middle cerebellar peduncles. The rest of the pons (the pontine tegmentum) contains a number of ascending and descending tracts as well as nuclei of the trigeminal nerve, abducens nerve, the facial nerve and the reticular formation. The facial colliculus is a bulge at the posterior aspect of the pons, where the facial nerve fibres wind round the abducens nerve nucleus. Most laterally in the pons is the nuclear complex associated with the vestibulocochlear nerve. A vascular lesion of the pons involving the facial colliculus will cause paralysis of the facial and abducens nerves resulting in ipsilateral facial palsy and convergent squint.
Cerebellum
The cerebellum (Fig. 8.8) is the largest part of the hindbrain. It is made up of two lateral cerebellar hemispheres separated by the vermis. The cerebellum is connected to the brainstem by the three pairs of cerebellar peduncles.
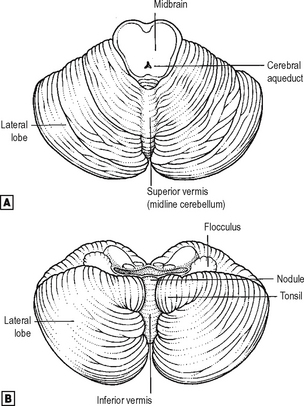
 superior view.
superior view.  inferior view.
inferior view.Meninges
The three layers of the meninges are:
The three meningeal spaces are:
Dura mater
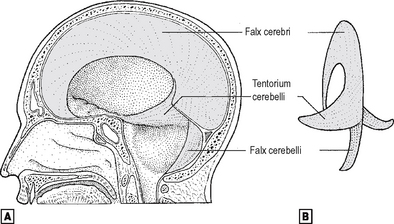
The cranial cavity is divided into compartments by three folds of dura mater. These folds are (Fig. 8.9):
 sagittal section of the head.
sagittal section of the head.  diagrammatic posterior view of the dural folds.
diagrammatic posterior view of the dural folds.Falx cerebri
Tentorium cerebelli
The tentorium cerebelli is attached anteriorly to the posterior clinoid process of the sphenoid bone, and its attachment runs posterolaterally along the superior border of the petrous temporal bone where the superior petrosal sinus is enclosed. Where the latter empties into the transverse sinus, the attached border turns posteromedially along the lips of the groove for the transverse sinus to reach the internal occipital protuberance and then continues on the opposite side of the skull to the other posterior clinoid process. The free border of the tentorium cerebelli is attached to the anterior clinoid process and, running posteriorly and then medially, it curves round the midbrain, forming the tentorial notch.
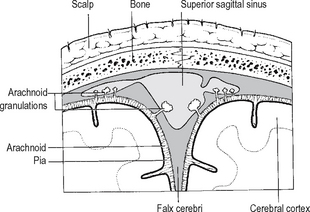
Arachnoid mater
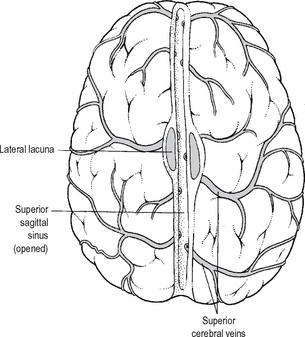
The smooth outer surface of the arachnoid mater is separated from the dura by the subdural space. The subarachnoid space between the arachnoid and the pia contains the cerebrospinal fluid and the major blood vessels. The arachnoid and the subarachnoid space extend into the vertebral canal and the sacral canal up to the level of the 2nd piece of sacrum. The deeper surface of the arachnoid gives delicate prolongations into the subarachnoid space. There are also prolongations, the arachnoid granulations which are the sites of reabsorption of CSF, into the superior sagittal sinus (Fig. 8.10) and probably into other venous sinuses.
Subarachnoid cisterns
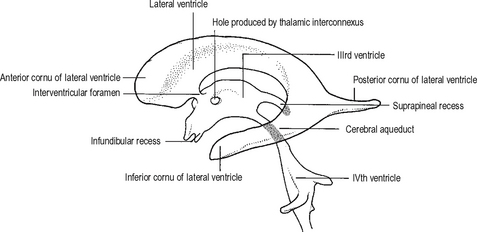
Ventricular system and cerebrospinal fluid
The general shape of the ventricular system is shown in Fig. 8.11. The lateral ventricles, larger than the others, are contained in the cerebral hemispheres. Each lateral ventricle has a body which is floored by the thalamus and the caudate nucleus. The corpus callosum forms its roof. The anterior horn projects forward in front of the interventricular foramen. The posterior horn projects into the occipital lobe, and the inferior horn projects into the temporal lobe. The choroid plexuses, which are found in the inferior horn and the body, are continuous with those on the roof of the third ventricle through the interventricular foramen. The interventricular foramen (foramen of Monro) is bounded by the anterior end of the thalamus and the fornix. It connects the lateral ventricle to the third ventricle.
BLOOD SUPPLY TO THE BRAIN
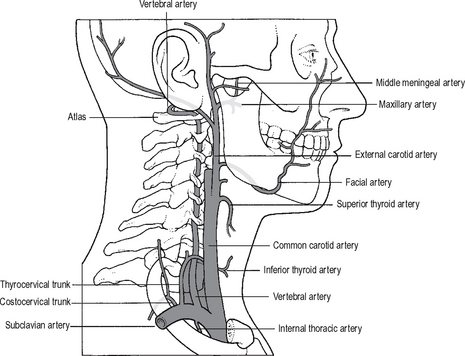
Arterial supply
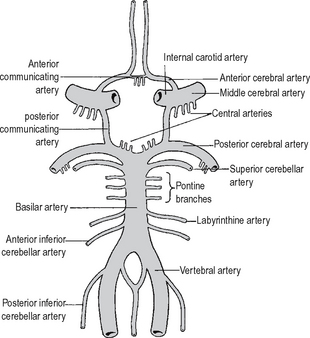
The two vertebral arteries and the two internal carotid arteries supply the brain (Fig. 8.12).
Vertebral arteries
The following branches supplying the brain and spinal cord arise from the vertebral artery:
The posterior spinal artery arises from the lower part of the vertebral artery, descends along the line of attachment of the dorsal roots of the spinal nerves and supplies the dorsal column of the white mater and the dorsal horn of the grey mater of the spinal cord. The artery often arises as a branch of the posterior inferior cerebellar artery.
Basilar artery
The following branches are given by the basilar artery:
The pontine arteries supply the pons.
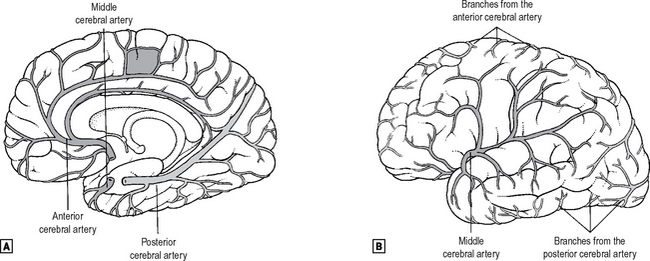
The posterior cerebral arteries are the terminal branches of the basilar artery. Each posterior cerebral winds round the midbrain to reach the medial surface of the cerebral hemisphere and supplies the occipital lobe, including the visual area, as well as the temporal lobe (Fig. 8.13). Occlusion of the posterior cerebral artery causes blindness in the contralateral visual field.
 medial view.
medial view.  lateral view.
lateral view.Internal carotid arteries
The branches of the internal carotid artery supplying the brain are as follows:
The anterior cerebral artery is the smaller of the two terminal branches of the internal carotid artery. It crosses over the optic nerve and, near the midline, is connected to the opposite artery by the anterior communicating artery. The anterior cerebral artery supplies the medial part of the inferior surface of the frontal lobe, and courses along the upper surface of the corpus callosum, supplying the medial surface of the frontal and parietal lobes and the corpus callosum. It also supplies a narrow strip on the upper part of the lateral surface. The motor and sensory areas of the lower extremity, located in this area (Fig. 8.5), are supplied by the anterior cerebral artery, resulting in characteristic paralysis when the artery is occluded.
Venous drainage of the brain
The superficial middle cerebral vein lies in the lateral sulcus. It runs downward and forward and drains into the cavernous sinus.
Cranial (dural) venous sinuses
The cranial venous sinuses (Fig. 8.15) are situated within the dura mater. They are devoid of valves and drain eventually into the internal jugular vein.
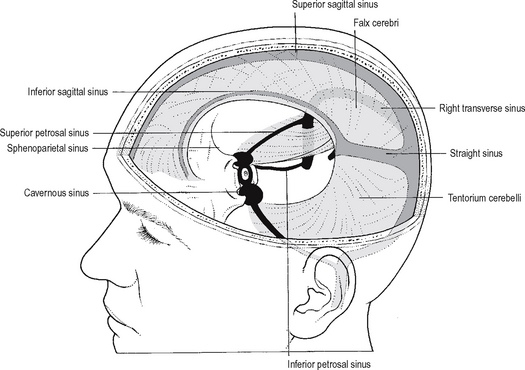
The cranial venous sinuses are:
The superior sagittal sinus begins in front of the crista galli, courses backwards along the attached border of the falx cerebri, and usually becomes continuous with the right transverse sinus near the internal occipital protuberance. At its commencement it may communicate with the nasal veins. A number of venous lacunae lie along its course and open into the sinus. The sinus and the lacunae are invaginated by arachnoid granulations. The superior cerebral veins drain into the superior sagittal sinus (Fig. 8.16).
The transverse sinus lies in the groove on the inner surface of the occipital bone along the posterior attachment of the tentorium cerebelli. On reaching the petrous temporal bone, it curves downwards into the posterior cranial fossa to follow a curved course as the sigmoid sinus.
Cavernous sinus
The cavernous sinus (Fig. 8.17), one on each side, situated on the body of the sphenoid bone, extends from the superior orbital fissure to the apex of the petrous temporal bone. Medially, the cavernous sinus is related to the pituitary gland and the sphenoid sinus. Laterally it is related to the temporal lobe of the brain. The internal carotid artery and the abducens nerve pass through the cavernous sinus. On its lateral wall from above downwards lie the oculomotor, trochlear and ophthalmic nerves. The maxillary divisions of the trigeminal go through the lower part of the lateral wall or just outside the sinus. The endothelial lining separates these structures from the cavity of the sinus.
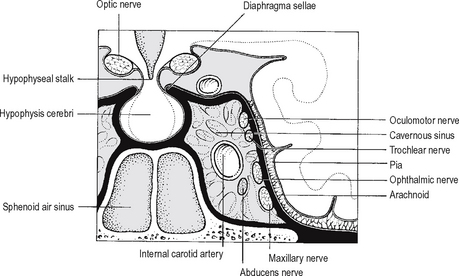
The connections of the sinus are illustrated in Fig. 8.15. Posteriorly, the sinus drains into the transverse/sigmoid sinus through superior petrosal sinus and via the inferior petrosal sinus, passing through the jugular foramen, into the internal jugular vein. The ophthalmic veins drain into the anterior part of the sinus.
Emissary veins passing through the foramina in the middle cranial fossa connect the cavernous sinus to the pterygoid plexus of veins and to the facial veins. The superficial middle cerebral vein drains into the cavernous sinus from above. The two cavernous sinuses are connected to each other by anterior and posterior cavernous sinuses lying in front of and behind the pituitary.
CRANIAL NERVES
I: Olfactory nerve
See also Chapter 13. Axons from the olfactory mucosa in the nasal cavity pass through the cribriform plate of the ethmoid to end in the olfactory bulb. A cuff of dura, lined by arachnoid and pia, surrounds each bundle of nerves, establishing a potential communication and a route of infection between the subarachnoid space and the nasal cavity.
III: Oculomotor nerve
The oculomotor nerve contains two major components:
Complete division of the third nerve results in:
The oculomotor nerve can be paralysed by:
A third nerve palsy with pupillary sparing often has an ischaemic or diabetic aetiology.
IV: Trochlear nerve
The trochlear nerve is the smallest of the cranial nerves. Its somatic motor fibres supply the superior oblique muscle. The nucleus of the trochlear nerve lies in the midbrain at the level of the inferior colliculus. From this nucleus axons pass dorsally around the cerebral aqueduct to decussate in the superior medullary velum. Each nerve then winds round the cerebral peduncle and passes forward in the interpeduncular cistern lying between the superior cerebellar and posterior cerebral arteries lateral to the oculomotor nerve. The nerve pierces the dura posterolateral to the oculomotor nerve, near the point where the free margin of the tentorium crosses the attached margin, to enter the cavernous sinus. It then lies in the lateral wall of the cavernous sinus below the oculomotor nerve and above the ophthalmic division of the trigeminal nerve. The nerve enters the orbit through the superior orbital fissure lateral to the tendinous ring from which the four recti take origin. It then turns medially over the optic nerve and, passing over the levator palpebrae superioris, reaches the superior oblique muscle which it innervates. When the trochlear nerve is injured, diplopia occurs on looking downwards. The patient complains of difficulty walking downstairs.
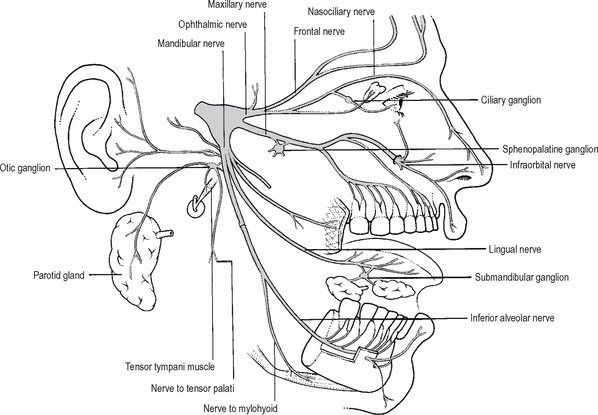
V: Trigeminal nerve
The trigeminal nerve (Fig. 8.18) is the principal sensory nerve of the head and it also innervates the muscles of mastication. Additionally, it is associated with four parasympathetic ganglia. Its distribution is as follows:
Nuclei of the trigeminal nerve
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


