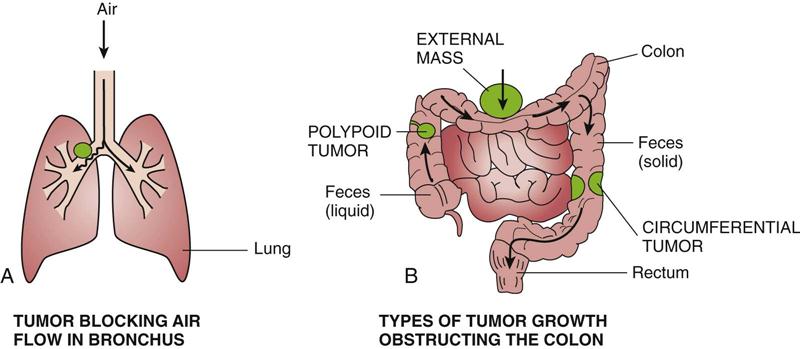
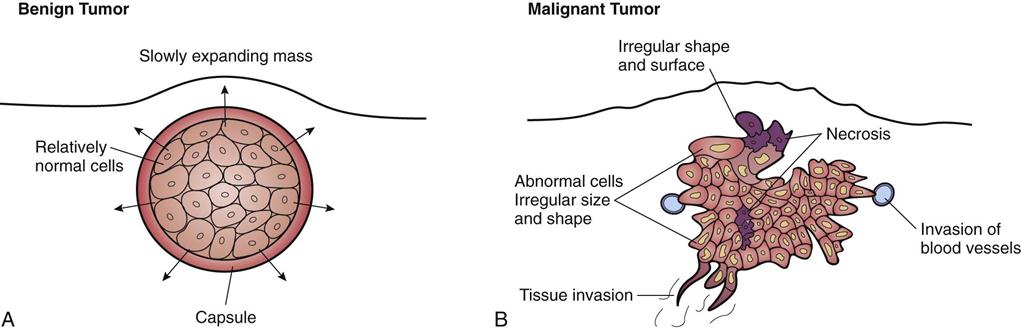
After studying this chapter, the student is expected to: 1. Distinguish between benign and malignant tumors, their characteristics, and terminology. 2. List the warning signs of cancer. 3. Explain the local and systemic effects of cancer. 4. Describe common diagnostic tests. 7. Explain the host defenses against cancer. 8. Discuss possible treatment measures, including radiation and chemotherapy, as well as nutrition. anemia angiogenesis antineoplastic apoptosis atypical biopsies chromosomes cytologic differentiation infiltrate leukopenia metastasis micrometastases mitosis mutation nadir oncology palliative pneumonia prognosis prophylactic radiofrequency ablation radioisotopes remission recurrence seeding thrombocytopenia total parenteral nutrition The cell is the functional and structural unit in the human body. Cells vary in their degree of development, depending on the differentiation or specialization required for a particular cell’s function; for example, neurons or cardiac muscle cells are highly developed, whereas fibroblasts are less so. Normally cells are organized in an orderly arrangement in a tissue and differentiated to fulfill that tissue’s purpose. When cells become disorganized or undifferentiated or their growth becomes uncontrolled, their specialized functions are lost. Every cell has an outer plasma membrane, enclosing the fluid cytoplasm or intracellular fluid. The membrane is semipermeable, controlling passage of materials into and out of the cell. It also maintains the cell’s shape. The nucleus of the cell consists of DNA, the genetic material that controls the particular cell’s function and structure, enclosed in the nuclear membrane. The cytoplasm contains various nutrients, proteins, glucose, and electrolytes required for cell metabolism. Additional substances are present, depending on the cell’s function; for example, glycogen in liver cells or lipids in fat cells. Other structures are located in the cytoplasm, such as ribosomes, granules that produce proteins; mitochondria providing energy in the form of ATP for cell activities; lysosomes containing digestive enzymes, to break down unwanted materials; and the Golgi complex to process and release proteins. Organelles inside the cell have many metabolic functions, such as the synthesis of protein or transport of cell products and wastes outside the cell membrane. The plasma membrane includes special protein molecules or receptors for substances such as hormones, chemical transmitters, or drugs, which affect the cell’s function. Cells may communicate with each other by chemicals or by forming protein channels between cells. Research is focused on this communication, seeking to learn the “what and how” of the transfer between cells and whether this knowledge could lead to the prevention of some diseases or new treatments. Cell membranes also have specialized mechanisms to adhere to each other and maintain an organized arrangement in a tissue or organ. Regulator genes control mitosis for different types of cells. Growth factors such as cytokines signal proliferation, whereas inhibitors inside cells prevent excessive growth. During its lifespan, each cell follows the basic cell cycle of growth and reproduction or mitosis. (See Fig. 20-10 for a schematic drawing of the cell cycle.) The timing of each event varies with the specific cell type. Epithelial cells that reproduce rapidly may complete the cycle in a few hours. Other cells spend months completing one cycle. Genetic control over growth and reproduction is exerted through DNA, and the daughter cells are identical to the parent cell. If DNA is altered in the parent cell, this mutation is passed on to the daughter cells. Different cells experience different life spans; for example, erythrocytes live for approximately 120 days, but some leukocytes survive only a few days. Highly specialized cells such as neurons cannot undergo mitosis, but they have a long life span of many years. Epithelial cells usually replicate very rapidly because of the demand for replacement caused by constant “wear and tear” on surface tissues. There are usually several layers of tightly packed cells, the upper layers being sloughed off or shed and replaced by regenerating cells from the lower layers. Some types of cells can increase their reproductive rate on demand; for example, bone injury increases osteoblast activity. Cell reproduction always requires an adequate blood supply to the area and sufficient quantities of essential nutrients such as amino acids, glucose, and oxygen. Normally, cell growth and reproduction are also subject to stimuli such as hormones and inhibition by contact with nearby cells. 20-1 Apply Your Knowledge Discuss several ways by which the normal process of cell replication can be altered, and state outcomes. Cellular aging occurs naturally over time and results in an altered structure of the cell, decreased function, and, in time, cell death. The processes of cellular aging and changes in cell control systems are not fully understood. Certain cells undergo apoptosis, programmed cell death (see Chapter 1). Current theories on the aging process focus on a programmed number of reproductive cycles available for a specific cell type and the effects of wear and tear causing cell damage (see Chapter 24). Changes in DNA can alter cell structure and function or cause cell death. DNA can mutate spontaneously during mitosis or as a result of exposure to chemicals, viruses, radiation, and other environmental hazards. Rapid rates of mitosis associated with tissue trauma or other stimuli may increase the risk of errors occurring in the chromosomes, cell enzymes, or cell components. Mutant cells may change function as well as lose control of mitosis. Seriously defective cells usually die or are destroyed by the immune system. A neoplasm or tumor is a cellular growth that is no longer responding to normal body controls. The cells continue to reproduce when there is no need for them. This excessive growth deprives other cells of nutrients. Many neoplasms are unable to function as normal tissue cells because they consist of atypical (abnormal) or immature cells. The characteristics of each tumor depend on the specific type of cell from which the tumor arises, resulting in a unique appearance and growth pattern. The expanding mass creates pressure on surrounding structures. Tumors are named according to a system (Table 20-1). The root word, such as chondro, is the cell of origin, in this case cartilage. Depending on the type of tissue in which a tumor is located, the suffix indicates malignant tumors (carcinoma for epithelial tissue, sarcoma for connective tissue). The suffix oma alone indicates a benign tumor, e.g., lipoma. However, a number of neoplastic disorders have acquired unique names that are recognized in medical practice. Examples include Hodgkin disease, Wilms tumor, and leukemia. Oncology is the study of malignant tumors, otherwise known as cancer. TABLE 20-1 Characteristics of specific tumors vary considerably depending on the cell of origin. The general characteristics of each type are summarized in Table 20-2. Benign tumors usually consist of differentiated cells that reproduce at a higher than normal rate. The benign tumor is often encapsulated and expands but does not spread (Fig. 20-1). It is usually freely moveable on palpation. Tissue damage results from compression of adjacent structures such as blood vessels. A benign tumor is not considered life threatening unless it is in an area such as the brain where the pressure effects can become critical. TABLE 20-2 Characteristics of Benign and Malignant Tumors By comparison, malignant tumors are usually made up of undifferentiated, nonfunctional cells that do not appear organized. The cells tend to reproduce more rapidly than normal and often show abnormal mitotic figures. These cells have lost cellular connections with each other, and reproduction is not inhibited in the presence of other similar cells. Tumor cells infiltrate or spread into surrounding tissue and may easily metastasize or break away to spread to other organs and tissues (Fig. 20-2). A tumor manifests as an enlarging space-occupying mass composed of more primitive or dysplastic cells. Normal organization, growth inhibition, contact controls, and cell-cell communication are absent. Cell membranes, including surface antigens, are altered. The expanding mass compresses nearby blood vessels, leading to necrosis and an area of inflammation around the tumor, and increases pressure on surrounding structures. Malignant cells do not adhere to each other but often break loose from the mass, infiltrating into adjacent tissue. Tumor cells often secrete enzymes such as collagenase, which break down protein or cells, adding to the destruction and facilitating the tumor’s spread into adjacent tissue. Inflammation and the loss of normal cells lead to a progressive reduction in organ function. As a tumor mass enlarges, the inner cells are frequently deprived of blood and nutrients and die. This necrosis can lead to more inflammation and infection at the site. Some cancer cells secrete growth factors, which stimulate angiogenesis, the development of new capillaries in the tumor, thus promoting tumor development. Antiangiogenesis factors have also been located and several new drugs are based on this blocking action. These drugs are of limited effect in clients receiving chemotherapy because the reduction in blood vessel development impairs the delivery of chemotherapy agents to the tumor. Tumor cells may increase the uptake of nutrients or “trap” nutrients, depriving normal cells and preventing any tissue regeneration. Some neoplasms develop very rapidly, whereas others remain in situ for a long time. In situ refers to neoplastic cells in a preinvasive stage of cancer that may persist for months or years. This condition offers an excellent opportunity for early diagnosis of cervical cancer and certain oral cancers. Grading of tumors is based on the degree of differentiation of the malignant cells—a grade I tumor has well-differentiated cells similar to the original cells, whereas a grade IV tumor is undifferentiated with cells varying in size and shape (anaplasia); this type of tumor is considered highly malignant and likely to progress quickly. All health care workers should be aware of the early indicators of possible malignancies. The classic warning signs of cancer are listed in the box below. Warning Signs of Cancer 1. Unusual bleeding or discharge anywhere in the body. 2. Change in bowel or bladder habits (e.g., prolonged diarrhea or discomfort). 3. A change in a wart or mole (i.e., color, size, or shape). 4. A sore that does not heal (on the skin or in the mouth, anywhere). 6. Anemia or low hemoglobin, and persistent fatigue. 7. Persistent cough or hoarseness without reason. 8. A solid lump, often painless, in the breast or testes or anywhere on the body. Even if cancer is not present, any of these signs could be the indicator of some other disease process, so it should be checked by a physician. A critical observation can save a life. Sometimes a client may need encouragement to have such warning signs investigated. • Pain is not usually an early symptom of cancer; rather, it occurs when the tumor is well advanced. Pain is a warning of a problem; therefore it is helpful if it occurs early, but this is rare. The severity of the pain depends on the type of tumor and its location. Pain may be caused by direct pressure of the mass on sensory nerves, particularly where space is restricted (e.g., bone cancer). Dull, aching pain results from the stretching of a visceral capsule such as occurs in the kidney or liver. Inflammation also contributes to pain because of increased pressure on the nerves and the irritation of nerve endings by chemical mediators (see Chapter 5). Secondary causes of pain include infection, ischemia, and bleeding. Blood can be “irritating” to tissues and, if it collects in an area, can cause pressure on nerves (see Chapter 4). • Obstruction can result when a tumor compresses a duct or passageway from an external position or grows inside a passageway or around a structure (Fig. 20-3). Obstruction may occur in ducts or tubes in the body such as those in the digestive tract. Blood supply or lymphatic flow may be restricted, leading to ulceration and edema. Air flow in the bronchi or nerve conduction may be blocked. Obstructions can cause serious complications for the patient, even in the early stage. In the late stage prevention of obstruction may form the rationale for continuing palliative treatment. Systemic or general effects of cancer include the following: • Bleeding may occur because the tumor cells may erode the blood vessels or cause tissue ulceration. Bone marrow depression and hypoproteinemia may contribute to poor clotting. Chronic bleeding is common in the digestive tract, where the mucosa fails to regenerate quickly. Chronic blood loss leads to iron deficiency anemia (see Chapter 10). Tests are important in the early detection of cancer and in long-term monitoring of the patient subsequent to the diagnosis. Routine screening tests and self-examination programs need to be promoted, especially in high-risk clients. Frequent monitoring during and after treatment as well as ongoing follow-up are important in assessing the effectiveness of treatment and providing warning of recurrence. A diagnostic test is not usually 100% reliable by itself because there may be false-negative or false-positive results. The only definitive test for malignancy requires examination of the tumor cells themselves. Other results should be assessed in conjunction with associated data. The following are selected types of tests used for the diagnosis of cancer: 3. X-ray, ultrasound, magnetic resonance imaging and computed tomography (CT) scans are methods of examining changes in tissues or organs (see Ready Reference 5 for information on these tests). In some cases radioisotopes may be used during these procedures to trace metabolic pathways and assess function.
Neoplasms and Cancer
Learning Objectives
Key Terms
Review of Normal Cells

Benign and Malignant Tumors
Nomenclature
Root
Suffix
Example
Fatty tissue: lip-
Benign: -oma
Lipoma: benign tumor of fatty tissue
Gland tissue: adeno-
Malignant epithelial tissue: -carcinoma
Adenocarcinoma: malignant tumor of epithelial lining of a gland
Fibrous tissue: fibro-
Malignant connective tissue: -sarcoma
Fibrosarcoma: malignant tumor of fibrous tissue
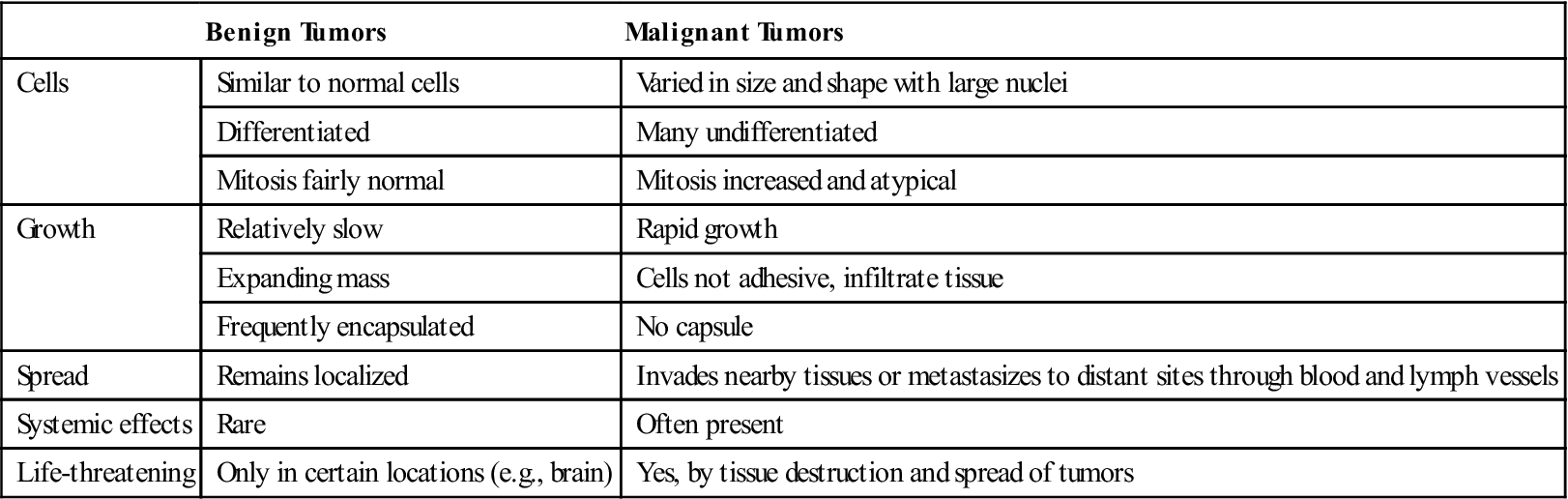
Characteristics of Benign and Malignant Tumors
Benign Tumors
Malignant Tumors
Cells
Similar to normal cells
Varied in size and shape with large nuclei
Differentiated
Many undifferentiated
Mitosis fairly normal
Mitosis increased and atypical
Growth
Relatively slow
Rapid growth
Expanding mass
Cells not adhesive, infiltrate tissue
Frequently encapsulated
No capsule
Spread
Remains localized
Invades nearby tissues or metastasizes to distant sites through blood and lymph vessels
Systemic effects
Rare
Often present
Life-threatening
Only in certain locations (e.g., brain)
Yes, by tissue destruction and spread of tumors
Malignant Tumors: Cancer
Pathophysiology
Effects of Malignant Tumors

Local Effects of Tumors
Systemic Effects of Malignant Tumors
Diagnostic Tests




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


