Hepatic TB seen in ∼ 1% of patients with active TB
More common in HIV(+) patients
Etiology/Pathogenesis
• Transmission typically by inhalation
Can reach liver by hematogenous spread or direct spread from GI tract
Clinical Issues
• Liver is usually involved as part of disseminated TB
• Most common symptoms overall are hepatomegaly, fever, abdominal pain, weight loss
• Tuberculoma/localized disease can mimic neoplasm and compress biliary tract, vessels
• Mortality ranges from 10-40%
Worse prognosis with immune compromise, drug-resistant organisms
Microscopic
• Numerous granulomas ± central necrosis
Coalescence of granulomas can produce tuberculoma
• Immunocompromised patients may have poorly developed granulomas or abscesses
• Acid-fast stains (+) in up to 60% of cases
Ancillary Tests
• Culture is more likely to be positive in cases with caseating necrosis
May take weeks to grow
• PCR has 53-88% sensitivity and 96-100% specificity
Diagnostic Checklist
• Have high index of suspicion in patients with hepatomegaly, fever, respiratory symptoms, and elevated liver tests, especially if patient is from endemic area
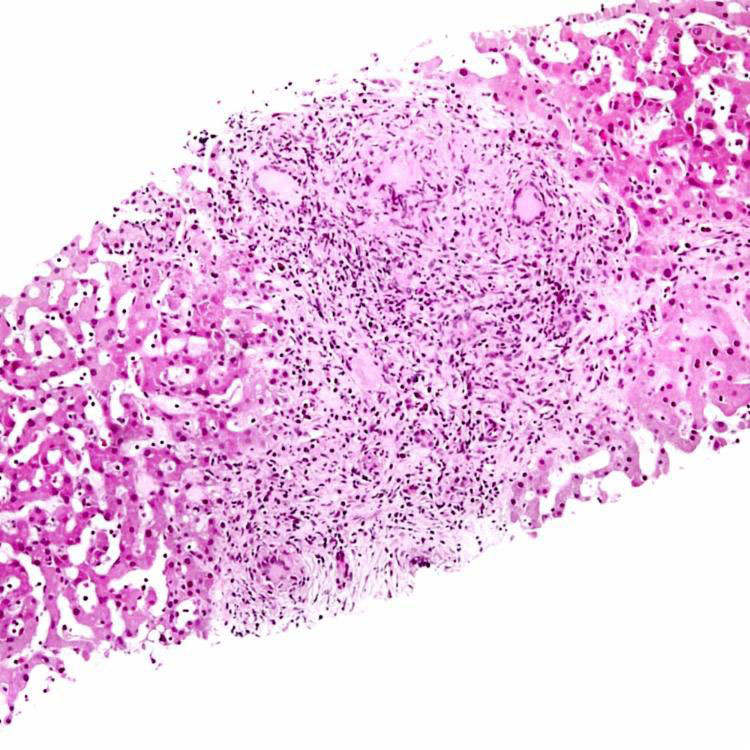
Granuloma With Giant Cells This liver biopsy in hepatic tuberculosis shows an expansile, portal-based granuloma with associated lymphocytes and giant cells. Note that the granuloma effaces the normal architecture of the liver.
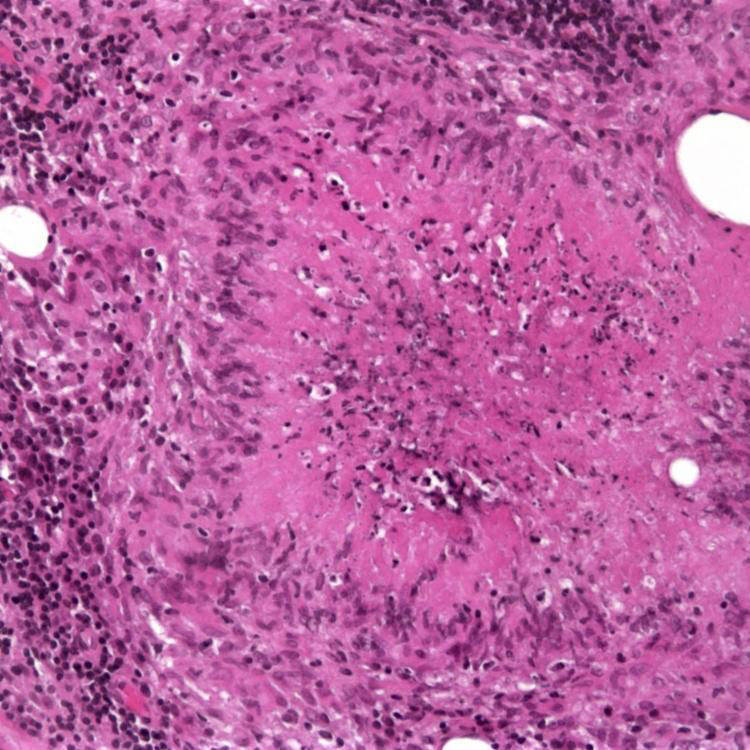
Caseating Necrosis This patient with disseminated tuberculosis had granulomas with central amorphous granular material, typical of caseating necrosis, within the liver and portal lymph nodes. Note the surrounding palisading histiocytes.
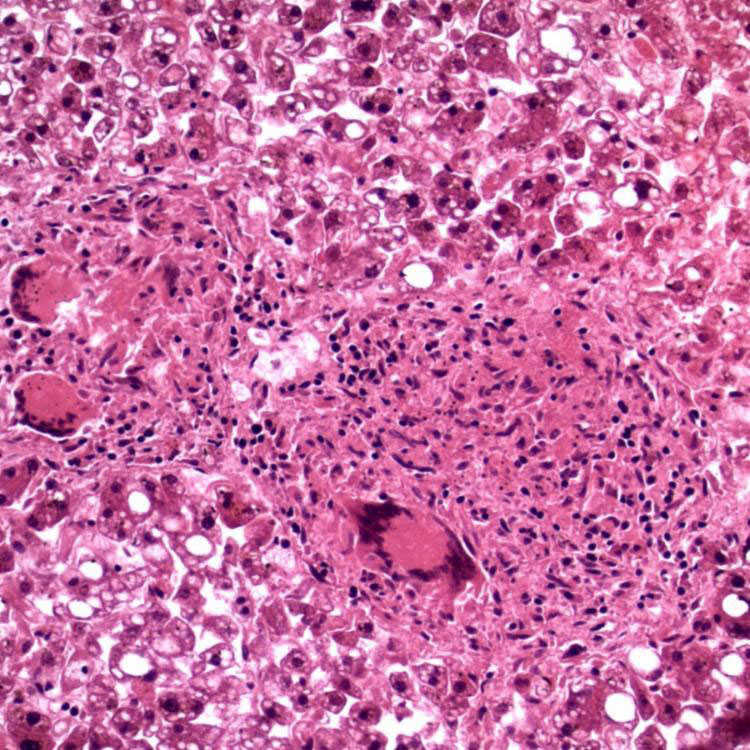
Miliary Tuberculosis in Liver The liver from an autopsy of a patient with miliary tuberculosis shows a small granuloma with associated lymphocytes and multinucleated giant cells and very focal eosinophilic granular necrotic debris.
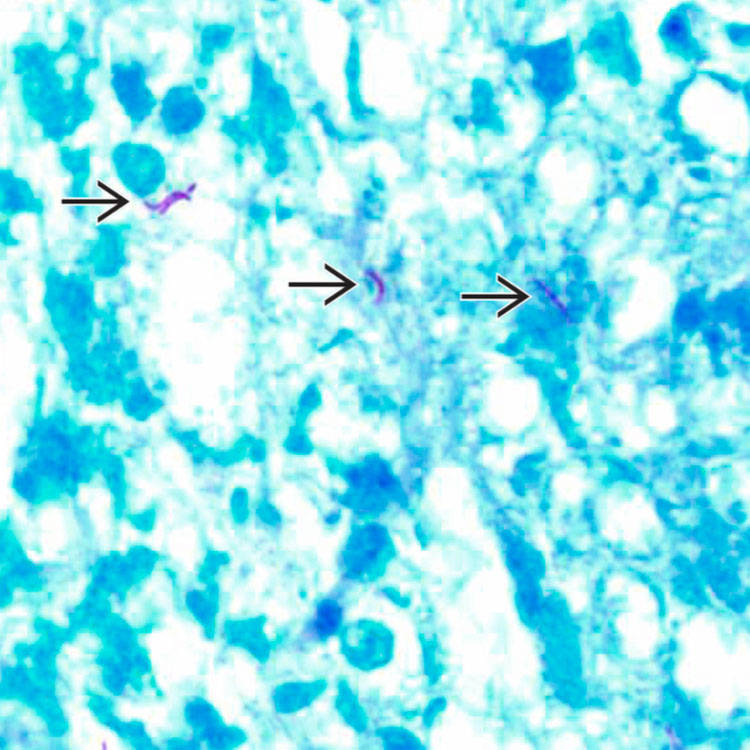
AFB Stain Acid-fast stain shows a few acid-fast bacteria with a slender, beaded appearance consistent with Mycobacterium tuberculosis.
TERMINOLOGY
Abbreviations
• Mycobacterium tuberculosis (MTB)
• Tuberculosis (TB)
Definitions
• Infection by MTB
∼ 8.5 million people develop TB annually; extrapulmonary TB is increasing in frequency
– Hepatic TB seen in ∼ 1% of patients with active TB
– More common in HIV(+) patients
ETIOLOGY/PATHOGENESIS
Environmental Exposure
• Transmission typically by inhalation
Can reach liver by hematogenous spread or direct spread from GI tract
Only gold members can continue reading. Log In or Register to continue





 with a slender, beaded appearance consistent with Mycobacterium tuberculosis.
with a slender, beaded appearance consistent with Mycobacterium tuberculosis.





