Chapter 17 A. Donor negative/recipient positive. B. Donor positive/recipient positive. C. Donor negative/recipient negative. D. Donor positive/recipient negative. E. The risk is equal for all donor/recipient matches. 2. A 3-year-old girl presented to the pediatric emergency department (ED) in the autumn, with fever and symptoms consistent with bronchiolitis. A rapid enzyme immunoassay (EIA) was positive for the etiologic agent (Figure 17-1). Which one of the following microorganisms is most likely to cause this infection? B. Rotavirus. C. Respiratory syncytial virus (RSV). D. Bordetella pertussis. E. Coronavirus. 3. A 30-year-old immune-competent male patient presented to his physician in the winter with a high fever, headache, myalgias, and nonproductive cough. A chest radiograph revealed a right lower lobe infiltrate. On hospitalization, broad-spectrum antibiotics were instituted, but his symptoms persisted. Which one of the following is the most likely etiologic agent? B. Streptococcus pneumoniae. C. Influenza A. D. Adenovirus. E. Parainfluenza. 4. A 47-year-old male kidney transplant patient presented with a low-grade fever, myalgias, and mild gastroenteritis. BK virus was suspected to be the etiologic agent of infection. Which one of the following statements is true regarding BK viruses? A. Most individuals have never been exposed to BK virus. B. BK virus can remain latent in the kidney and uroepithelial cells. C. The assay used for early diagnosis of BK nephropathy is a qualitative (polymerase chain reaction) PCR assay using urine. D. Antiviral therapy is used empirically before transplantation. E. BK virus is ubiquitous, causing infections in all solid-organ transplant patients. 5. A 28-year-old man was recently diagnosed with HIV-1 infection. His baseline viral load was 204,000 copies/mL and he was started on a highly active antiretroviral therapy (HAART) regimen. One week later, a repeat viral load was 98,000 copies/mL. Which one of the following statements would best describe his condition? B. He has not responded to treatment because his viral load remains unchanged. C. His HAART regimen should be modified because there was no significant change in viral load. D. He should continue on HAART and the viral load test should be repeated immediately. E. He should continue on HAART and his viral load should be measured in 2 to 8 weeks. 6. A 36-year-old woman with a history of intravenous drug abuse was referred for follow-up due to abnormal liver function tests. The result of her hepatitis C virus (HCV) quantitative PCR test was positive. Which one of the following statements best describes the clinical utility of ordering an HCV genotype assay? A. To confirm the diagnosis of HCV infection. B. To detect HCV and human immunodeficiency virus coinfection. C. To monitor antiviral therapy. D. To predict duration of antiviral therapy. E. To determine viral load. 7. A 32-year-old recent HIV-positive immigrant from Vietnam presented to the ED with fever, weight loss, and lymphadenopathy. Two sets of blood cultures were collected and became positive after 2 days of incubation. The organism demonstrated in Figure 17-2 was recovered after 72 hours of incubation at 30°C. Which one of the following is the etiologic agent? B. Aspergillus nidulans. C. Trichophyton rubrum. D. Fusarium solani. E. Cryptococcus neoformans. 8. A 13-year-old female bone marrow transplant patient presents with nasal congestion and a severe headache. A needle aspirate from the sinus reveals hyphae by light microscopy (Figure 17-3). Which one of the following infections is highest on the differential diagnosis? B. Aspergillosis. C. Candidiasis. D. Mycetoma. E. Rhinosporidiosis. 9. A 10-year-old boy presents with a 6-month history of progressive hepatomegaly. His mother was positive for chronic hepatitis B virus (HBV) during her pregnancy. Laboratory testing on the child reveals positive HBV surface antigen, negative HBV surface antibody, positive HBV core antibody, and HBV DNA 56,800 IU/mL. Which one of the following statements is true regarding HBV infection? A. He was exposed to HBV at birth, but the infection was transmitted horizontally. B. Active replication of HBV is occurring. C. His liver injury is related to actively replicating HBV in hepatocytes. D. His HBV core antibody is positive, indicating his infection has cleared. E. HBV disease is more severe in children than adults. 10. A 25-year-old injection drug user presented to the ED with flulike symptoms, including decreased appetite, fever, fatigue, and headache. He admitted to recent episodes of unprotected sex with both men and women. The patient had a positive HIV 1/2 EIA result; however, the Western blot assay was negative. Which one of the following tests is required to establish a diagnosis? B. HIV genotyping. C. HIV quantitative PCR. D. HIV qualitative PCR. E. Human herpesvirus 8 (HHV-8) PCR. 11. A 72-year-old man from Staten Island, New York, presented in the summer with headache, nuchal rigidity, and fever. The diagnosis was made by serology and confirmed by PCR. Which one of the following is the most likely agent of infection? B. Cryptococcus neoformans. C. West Nile virus (WNV). D. Naegleria fowleri. E. Parvovirus B19. 12. A 30-year-old man presented to a sexually transmitted disease clinic with a 1-week history of genital lesions. A swab sample of the lesion was collected and transported in viral transport medium to a virology laboratory for herpes virus detection. Same-day detection of herpes simplex viruses (HSV) can be accomplished using which one of the following methods? A. The cytopathic changes observed in the cultured cells can distinguish HSV types 1 and 2. B. Infected cells can be visualized after staining with virus-specific, fluorescently labeled antibodies. C. Shell vial culture followed by the detection of specific HSV proteins in the infected cells using monoclonal antibodies. D. Type-specific HSV serological testing. E. Reverse transcriptase (RT)-PCR assay for detecting HSV types 1 and 2. 13. Infections by which one of the following viruses is not vaccine preventable? B. RSV. C. Measles virus. D. Rotavirus. E. Rubella virus. 14. Which one of the following statements regarding the laboratory diagnosis of influenza infection is correct? B. Rapid EIAs are the most sensitive diagnostic tool. C. Infected patients shed influenza virus for 24 hours after the onset of symptoms. D. Rapid EIAs are available for influenza A, but not influenza B. E. If the patient has received an annual influenza vaccine, then infection will be prevented. 15. An 8-month-old girl presented to the ED with multiple vesiculopustular lesions over her body and a fever of 39°C. One of the lesions was sampled and a diagnosis was made within hours (Figure 17-4). Which one of the following is the etiologic agent in this case? A. Varicella zoster virus (VZV). B. Coxsackievirus A. C. Streptococcus pyogenes. D. Coxsackievirus B. E. Human herpes virus 6 (HHV-6). 16. A 48-year-old woman presented to her physician with an erythematous rash on one side of her body. She also has clusters of small vesicles in the same region. Before the rash appeared, she experienced “burning” pain and the area was tender to palpation. A vesicle was sampled and the laboratory confirmed the diagnosis within 3 hours. Which one of the following is the etiologic agent? B. Herpes simplex virus. C. Parvovirus B19. D. Varicella zoster virus (VZV). E. Measles virus. 17. A 41-year-old healthy man donated blood at a local Red Cross. A week later, he received a blood screening test report indicating his hepatitis B core antibody (HBcAb) test was positive. He was referred to a liver disease specialist for additional evaluation. Additional test results showed that the patient was hepatitis B surface antigen (HBsAg) negative, hepatitis B surface antibody (HBsAb) positive, and hepatitis anti-core IgM negative. Which one of the following statements best describes the man’s current status with regard to hepatitis B virus (HBV)? B. Immune to HBV due to natural infection. C. Immune to HBV due to HBV vaccination. D. Chronic HBV infection. E. Susceptible to HBV infection. 18. Passengers on a cruise ship recently experienced an outbreak of norovirus; 40% of them presented to the medical clinic with vomiting and diarrhea. Which one of the following characteristics of this virus impacts the occurrence and control of outbreaks? A. Transmission via inhalation of respiratory droplets. B. Immunity related to prior vaccination. C. Immunity related to prior infection. D. Susceptibility of the virus to dilute bleach. E. Low infectious dose required for infection. 19. Which one of the following viruses is an enveloped, double-stranded DNA virus? B. Rhinovirus. C. Rotavirus. D. Influenza A virus. E. Herpes simplex virus type 2. 20. A 78-year-old man presented to his physician with a 24-hour history of fever, chills, and severe body aches. A rapid diagnostic test was performed in less than 30 minutes, and oseltamivir was prescribed based on the result. Which one of the following is the etiologic agent of the infection in this patient? B. Adenovirus. C. Influenza A virus. D. Haemophilus influenzae. E. Parainfluenza virus. 21. A 50-year-old woman presented to her local ED after recently returning from an extended vacation in the Dominican Republic. Her chief complaints included fever, headache, and malaise. She had been bitten by a dog 4 weeks earlier in the Dominican Republic, and the site was still painful. Which one of the following regimens is best for rabies prophylaxis? A. Chloramphenicol and rabies vaccine. B. Rabies immune globulin. C. Ribavirin and rabies vaccine. D. Rabies vaccine and rabies immune globulin. E. Rabies vaccine. 22. Which one of the following viruses is an enveloped, single-stranded RNA virus? B. Enterovirus 71. C. Parvovirus B19. D. Cytomegalovirus. E. Rotavirus. 23. A 3-month-old girl presents to her pediatrician with a maculopapular rash on her trunk, neck, and arms. Her mother reports that the child had a fever of 103°F 2 days earlier, which has since resolved. She is diagnosed with roseola. Which one of the following is the etiologic agent associated with this disease? B. Human herpes virus 6. C. Parvovirus B19. D. Coxsackievirus. E. Cytomegalovirus. 24. Which one of the following hepatitis C virus (HCV) genotypes is the most predominant in the United States? B. Genotype 2. C. Genotype 3. D. Genotype 4. E. Genotype 5. 25. An astute infection control practitioner observed that three recent admissions for pneumonia were referred from the same long-term care facility. All patients presented with fever, nonproductive cough, and lower lobe infiltrates. Respiratory secretions were collected for bacterial and viral cultures. A rapid amplification assay identified a DNA virus as the etiologic agent, and unnecessary antibiotic therapy was avoided. Which one of the following viruses caused these cases of viral pneumonia? B. Adenovirus. C. RSV. D. Parainfluenza virus. E. WNV. 26. At a routine well-child visit, it was recommended that a 14-year-old girl receive a vaccine to prevent infection with a sexually transmitted virus and its subsequent sequelae. Which one of the following answers best describes the type(s) of virus(es) that this vaccine protects against? A. Human papillomavirus types 6, 11, 16, and 18. B. HIV type 1. C. Adenovirus serotypes 7, 22, and 43. D. Herpes simplex virus type 2. E. Herpes simplex virus type 1. Major points of discussion ■ Approximately 40% to 90% of the general population is CMV seropositive, indicating previous exposure to CMV. ■ For the highest-risk patients (i.e., donor positive/recipient negative), prophylaxis is more successful for CMV disease prevention than preemptive therapy. ■ Transplant settings associated with the highest risk of CMV disease include heart, lung, and bone marrow transplantation. ■ CMV treatment can include intravenous ganciclovir or oral valganciclovir.13 2. A. Parainfluenza. Major points of discussion ■ RSV is an enveloped, single-stranded RNA virus that belongs to the family of paramyxoviruses. ■ RSV is a major cause of bronchiolitis in young children. ■ RSV can be rapidly detected directly from respiratory specimens using nucleic acid amplification technology. There are also rapid EIA kits for RSV detection. ■ There is no currently no vaccine available to prevent RSV infection. ■ Treatment is typically supportive and currently available antiviral agents are not effective.4 3. A. Mycoplasma pneumonia. Major points of discussion ■ The antiviral agents used to treat influenza A infections are amantadine, rimantadine, and oseltamivir. Oseltamivir is also effective for treating influenza B infections. ■ Influenza A destroys the tissue lining of the respiratory tract, inducing inflammation and predisposing the patient to secondary bacterial infections. ■ Rapid diagnostic tests for detection of influenza A include EIAs and real-time nucleic acid amplification assays. ■ Influenza A has two major surface antigens: hemagglutinin and neuraminidase. Antigenic drifts, due to point mutations in these proteins, necessitate yearly vaccinations. Antigenic shifts can cause pandemics due to major structural changes resulting from genetic reassortment between human and animal influenza A strains.11 4. A. Most individuals have never been exposed to BK virus. Major points of discussion ■ BK virus is a nonenveloped, double-stranded DNA virus in the Polyomavirus family group. ■ BK viral infection occurs in 1% to 10% of kidney transplant recipients and typically manifests in the first year following transplantation. ■ BK viral load is typically first detected in urine rather than in blood, and the levels of virus in urine can be used to predict viremia. ■ The quantitative real-time PCR assay is used to measure viral load in plasma and urine. ■ Therapeutic strategies, which often include the antiviral agent cidofovir, can result in good clinical success if BK nephropathy is diagnosed at an early stage.12 5. A. His treatment response was successful because his HIV-1 viral load was significantly reduced. Major points of discussion ■ A combination of several antiretroviral drugs, called HAART, has been very effective in reducing the replication of HIV in the bloodstream. ■ Treatment guidelines recommend that anyone with a viral load in blood of more than 100,000 copies/mL should begin treatment. ■ The Department of Health and Human Services Panel recommended that patients should be tested for HIV viral load 2 to 8 weeks after initiation of antiretroviral therapy and then 3 to 4 months thereafter. ■ Patient testing should be conducted at the same medical laboratory, using the same viral load test and analyzer, due to considerable variation in results using different test methods. ■ Baseline HIV viral load levels should be measured before initiating antiretroviral therapy. 6. A. To confirm the diagnosis of HCV infection. Major points of discussion ■ There are at least six major HCV genotypes (genotypes 1 to 6). ■ For patients with HCV genotypes 2 and 3, a 24-week course of combination treatment is adequate, whereas for patients with genotype 1, a 48-week course is recommended. ■ HCV genotype 1 (subtypes 1a and 1b) is the most common in the United States, followed by genotypes 2 and 3. ■ Less common HCV genotypes (i.e., genotypes 4 to 6) are beginning to be observed more frequently because of the growing cultural diversity within the United States. ■ HCV genotypes are determined by using direct sequence analysis of the 5’ noncoding regions of the HCV genome, or reverse hybridization analysis using genotype-specific oligonucleotide probes.8,9 7. A. Penicillium marneffei. Major points of discussion ■ P. marneffei demonstrates thermal dimorphism (i.e., mold at 30°C and yeast at 37°C) and growth is inhibited by cyclohexamide. ■ Transmission of P. marneffei is most likely airborne, via inhalation of conidia from an environmental reservoir (often associated with exposure to bamboo rats). ■ Other Penicillium spp. are not dimorphic and demonstrate septate hyphae in tissue, whereas P. marneffei are present in a yeast-like form. ■ P. marneffei is typically highly susceptible to miconazole, itraconazole, and ketoconazole but resistant to fluconazole. 8. A. Mucormycosis. Major points of discussion ■ The hyphae of the Mucorales fungi are nonseptate and branching is nondichotomous, irregular, and sometimes at right angles. ■ Mucormycosis can invade the lung, nasal, sinus, brain, and mucous membranes. ■ Fungi causing mucormycosis can be differentiated from aspergillosis by the morphology of the hyphae and by the presence of chlamydospores in the hyphae. ■ Differential characteristics of commonly encountered pathogens causing mucormycosis include rhizoid production and sporangiophore pigment (see table below). Characteristics of Representatives of Mucorales
Microbiology
Virology

Rationale: Although the clinical symptoms of infection with parainfluenza are similar to those of respiratory syncytial virus, no rapid EIA kits are currently available for its detection.
B. Rotavirus.
Rationale: Rotavirus infections cause diarrhea in children.
C. Respiratory syncytial virus (RSV).
Rationale: RSV is the most frequent cause of bronchiolitis. There are rapid EIA kits for RSV detection.
D. Bordetella pertussis.
Rationale: Patients present with paroxysms of coughing and there is no rapid EIA kit to detect this pathogen.
E. Coronavirus.
Rationale: Coronavirus is the etiologic agent of the common cold and presents with rhinitis and cough, not bronchiolitis; no rapid EIA kits are currently available to detect this virus.
Rationale: The typical presentation for M. pneumoniae, which causes “walking” or “atypical” pneumonia, is less severe and would have improved on antibiotics.
B. Streptococcus pneumoniae.
Rationale: S. pneumoniae is characterized by a productive cough, and an immunocompetent patient should have responded to antimicrobial therapy.
C. Influenza A.
Rationale: Influenza A is highest on the differential diagnosis in this setting due to the nonproductive cough, severity of presentation, and lack of response to antibiotics.
D. Adenovirus.
Rationale: Adenovirus infections more often present with pharyngitis and bronchiolitis.
E. Parainfluenza.
Rationale: Parainfluenza infections more often present with croup and bronchiolitis.
Rationale: More than 90% of the population has been infected with BK virus by 10 years of age.
B. BK virus can remain latent in the kidney and uroepithelial cells.
Rationale: BK virus establishes latency in the urogenital tract and reactivates during immunosuppressive therapy.
C. The assay used for early diagnosis of BK nephropathy is a qualitative polymerase chain reaction (PCR) assay using urine.
Rationale: The quantitative BK DNA PCR viral load assay is used for diagnosis and to monitor the response to therapy.
D. Antiviral therapy is used empirically before transplantation.
Rationale: Patients are treated only when BK infection has been diagnosed.
E. BK virus is ubiquitous, causing infections in all solid-organ transplant patients.
Rationale: BK virus can cause infection in either hematopoietic stem cell transplant or kidney transplant patients.
Rationale: A less than threefold reduction in viral load is not considered significant and may be due to biological variation.
B. He has not responded to treatment because his viral load remains unchanged.
C. His HAART regimen should be modified because there was no significant change in viral load.
Rationale: Since the patient has only been on HAART for a week, it is too early to predict the efficacy of the regimen.
D. He should continue on HAART and the viral load test should be repeated immediately.
E. He should continue on HAART and his viral load should be measured in 2 to 8 weeks.
Rationale for B, D, and E: It is recommended that patients have their HIV viral load quantified 2 to 8 weeks post initiation of antiretroviral therapy.6
Rationale: The diagnosis of HCV infection is based on the presence of HCV-specific antibodies and detectable virus in whole blood or plasma.
B. To detect HCV and human immunodeficiency virus coinfection.
Rationale: The HCV genotyping assay only detects HCV genomic targets.
C. To monitor antiviral therapy.
Rationale: The HCV RNA quantitative assay (i.e., HCV viral load) should be performed to monitor antiviral treatment.
D. To predict duration of antiviral therapy.
Rationale: Infection with HCV genotype 1, rather than genotypes 2 or 3, requires a longer course of treatment.
E. To determine viral load.
Rationale: The HCV RNA quantitative assay should be performed to determine the number of viral copies per milliliter of whole blood or plasma.
Rationale: P. marneffei produces a red diffusible pigment and microscopic morphology demonstrates flask-shaped phialides and chains of round conidia.
B. Aspergillus nidulans.
Rationale: A. nidulans does not produce a diffusible pigment and microscopic morphology demonstrates biseriate phialides and round conidia.
C. Trichophyton rubrum.
Rationale: T. rubrum does not produce a diffusible pigment and microscopic morphology demonstrates tear-shaped microconidia.
D. Fusarium solani.
Rationale: F. solani does not produce a diffusible pigment and microscopic morphology demonstrates sickle-shaped septated macroconidia.
E. Cryptococcus neoformans.
Rationale: C. neoformans is an encapsulated yeast and does not produce a diffusible pigment.
Rationale: Mucor spp. contain fungal elements that are largely nonseptate with irregular branching.
B. Aspergillosis.
Rationale: Aspergillus spp. have hyaline septate hyphae with branching at 45-degree angles.
C. Candidiasis.
Rationale: Candida spp. form pseudohyphae that show distinct constrictions at the septa and form budding yeast cells.
D. Mycetoma.
Rationale: Fungi and bacteria causing mycetoma appear as aggregates of intertwined filaments, rather than individual hyphae.
E. Rhinosporidiosis.
Rationale: Rhinosporidium seeheri invades mucocutaneous tissue and appears as round mature sporangia containing endospores.
Fungus
Rhizoids
Sporangiophores
Optimal Growth Temp (°C)
Pathogenicity
Rhizopus
Present
Unbranched, brown
45-50, inhibited by cycloheximide
Most common pathogen
Mucor
Absent
Branched, hyaline
≤ 37
Opportunistic, occasional
Rhizomucor
Few
Branched, dark brown
38-58
Opportunistic, occasional
Absidia (Lichtheimia)
Present
Fine branches, hyaline
45-50
Uncommon pathogen ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Microbiology: Virology
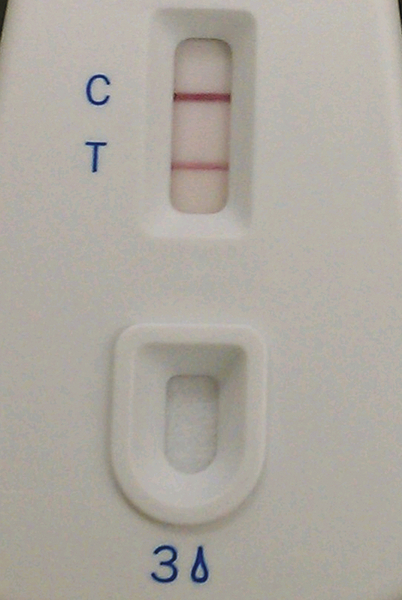
Figure 17-1 Enzyme immunoassay: C is the positive control and T is the sample.
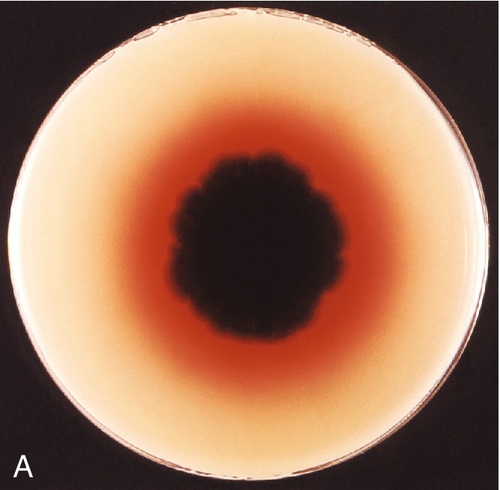
Figure 17-2 A, Reverse colony morphology on Sabouraud agar plate. B, Wet mount from growth at 30°C (× 100).
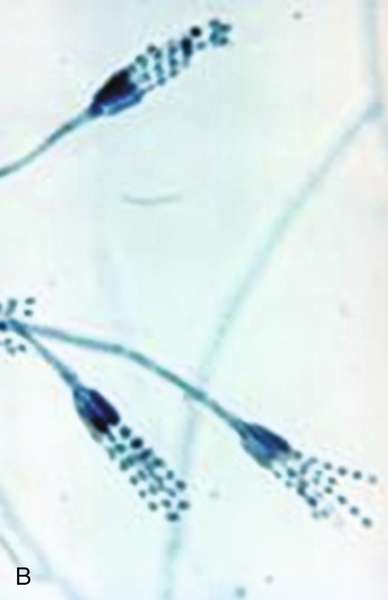
Figure 17-3 Methenemine silver stain of fungal elements.
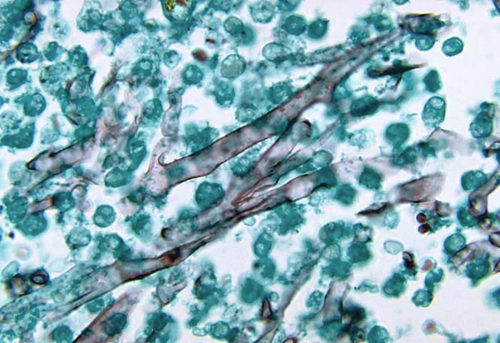
Figure 17-4 Vesiculopustular lesion on the cheek of an 8-month-old girl.
