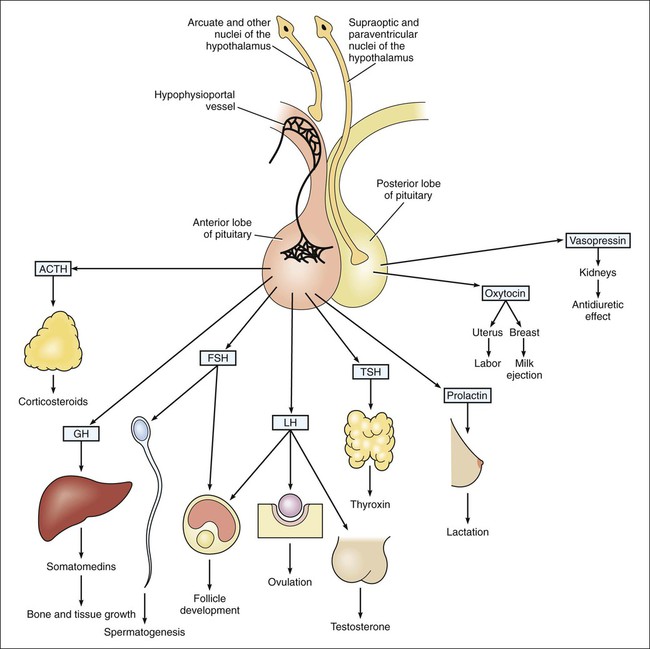
The adenohypophysis secretes six hormones: (1) corticotropin (adrenocorticotropic hormone [ACTH]); (2) somatotropin (growth hormone); (3) follicle-stimulating hormone (FSH); (4) luteinizing hormone (LH); (5) thyrotropin (thyroid-stimulating hormone [TSH]); and (6) prolactin. The actions of these anterior pituitary hormones are summarized in Figure 31-1.
Hypothalamic and Pituitary Drugs
Overview
Adenohypophysis and Hypothalamus
Anterior Pituitary Hormones
Corticotropin and Related Drugs
Growth Hormone and Related Drugs
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Hypothalamic and Pituitary Drugs
Only gold members can continue reading. Log In or Register to continue
