• Normal diastolic (<82 mm Hg) but elevated systolic pressure (>158 mm Hg) (increased pulse pressure) suggests decreased compliance of aorta (arteriosclerosis) and twofold increase in cardiovascular death rates. Other causes of increased pulse pressure are increased stroke volume from aortic regurgitation, thyrotoxicosis, fever. • Classification of hypertension by cause: >90% of cases are classified as essential hypertension—no discernable cause. Essential hypertension groups are based on level of renin (enzyme secreted by kidney juxtaglomerular cells, linked to aldosterone in negative feedback loop). Renin helps generate vasoconstricting peptide angiotensin II. Renin secretion is influenced by fluid volume and sodium (Na) intake. • Low-renin essential hypertension involves low renin activity. Aldosterone production is not being suppressed, leading to mild hyperaldosteronism with Na retention, increased fluid volume, and increased BP. This also occurs with normal-renin hypertension; low-renin hypertension may be at the end of the continuum with essential hypertension. Patients with low renin levels have increased sensitivity to angiotensin II. • Normal-renin essential hypertensives typically are insulin resistant with abdominal obesity. Hyperinsulinemia and insulin resistance are present even in lean hypertensives without non-insulin-dependent diabetes mellitus, suggesting a strong relation between insulin sensitivity and BP. Because insulin modifies ion transport across cell membranes, insulin insensitivity de-creases cytosolic magnesium (Mg) and increases cytosolic calcium (Ca) in vascular smooth muscle, increasing vascular reactivity. Normal-renin essential hypertensives typically do not respond to Na restriction. • High-renin essential hypertensives comprise 15% of essential hypertension patients. Renin elevation (and high BP) may arise from increased adrenergic system activity. • Categories based on renin can identify therapeutic interventions, but renin levels do not remain constant in a given patient. In low-renin essential hypertension caused by insulin resistance secondary to obesity, weight loss regains insulin sensitivity but BP may not normalize. The patient would then have normal- or high-renin essential hypertension. I Essential hypertension (>90% of all cases of hypertension) B Acute and chronic glomerulonephritis D Renovascular stenosis or renal infarction E Most other severe renal diseases (e.g., arteriolar nephrosclerosis, diabetic nephropathy) A Adrenocortical hyperfunction B Cushing’s disease and syndrome D Congenital or hereditary adrenogenital syndromes (17-hydroxylase and 11-hydroxylase defects) C Familial dysautonomia (Riley-Day) D Polyneuritis (acute porphyria, lead poisoning) E Increased intracranial pressure (acute) • “White coat” hypertension: persistent elevation of BP only at clinic or physician’s office. Prevalence may be 20%-45% of diagnosed hypertensives; is more frequent in women, older patients, and persons with mild hypertension. This should not be confused with “white coat effect”—the difference in BP between office and daytime ambulatory BP that occurs in patients with white coat hypertension and other causes. Treat white coat hypertension as if it were essential hypertension; it mirrors real-life reactions to stress. It is not an innocent phenomenon because it is linked to higher mortality and twice the risk of developing sustained hypertension as normotensives. • Ambulatory BP monitoring: clinically useful for assessing suspected white coat hypertension and cardiovascular risk. If white coat hypertension is confirmed, drug treatment is not indicated; treat with lifestyle and dietary modification, weight reduction, exercise, smoking cessation, and correction of glucose and lipid abnormalities. Follow-up with semiannual or annual ambulatory BP monitoring. • Etiology: vascular, hormonal, renal, and neurologic factors function in complex interrelations to maintain normal BP. Disruption of any single facet creates a cascading effect on regulatory mechanisms. Genetic factors play a role, but dietary, lifestyle, psychological, and environmental factors are underlying causes. Dietary factors: obesity; high Na/potassium (K) ratio; low-fiber, high-sugar diet; high saturated fat and low omega-3 fatty acid intake; low calcium, magnesium, and vitamin C intake. Lifestyle factors: stress, lack of exercise, smoking. From 40% to 60% of hypertensives are Na sensitive. The heavy metals lead (Pb), mercury, cadmium, and arsenic target kidneys as end organs. Bone lead studies indicate that exposure to heavy metals is linked to increased risk for hypertension. • Antihypertensive drugs: diuretics, beta-blockers, ACE inhibitors, calcium channel blockers. • Diuretics: lower BP by reducing fluid volume in blood and tissues by promoting elimination of salt and water by increased urination. They relax smaller arteries, allowing them to expand and increase fluid capacity of arterial system. Types of diuretics: thiazides, loop diuretics, and potassium-sparing diuretics. Thiazides are more effective in lowering BP than are loop and potassium-sparing diuretics, allowing lower, safer dosing. Side effects: lightheadedness; increased blood sugar and uric acid (aggravation of gout); muscle weakness and cramps caused by low K; decreased libido; impotence; allergic reactions, headache, blurred vision, nausea and vomiting, diarrhea. Loss of K, Mg, and Ca help lower BP and prevent MI. The drugs also increase cholesterol and triglycerides, increase blood viscosity, raise uric acid, and increase platelet stickiness. Thiazides may increase risk of MI or stroke and worsen blood sugar control (difficult for diabetics). • Beta-blockers: block binding of catecholamines on beta-receptors, reducing rate and force of heart contraction and relaxing arteries; treat angina and certain heart rhythm disturbances. Long-term inhibition of heart function can lead to heart failure. They fail to reduce cardiovascular mortality rate and increase risk of developing diabetes. Side effects: reduced cardiac output in relaxed arteries causes cold hands and feet, nerve tingling, impaired mental function, fatigue, dizziness, depression, lethargy, reduced libido, and impotence. They raise cholesterol and triglycerides. Beta-blocker treatment must not be discontinued suddenly because of withdrawal syndrome—headache, increased heart rate, greatly increased BP. • Calcium channel blockers and ACE inhibitors: better tolerated than diuretics and beta-blockers. Calcium channel blockers lower risk for strokes and increase risk for MI. • Calcium channel blockers: block normal passage of Ca through channels in cell membranes, slowing nerve conduction and inhibiting muscle contraction. They reduce rate and force of heart contraction, relax arteries, and slow heart nerve impulses. Side effects: constipation, allergic reactions, fluid retention, dizziness, headache, fatigue, impotence, disturbances of heart rate or function, heart failure, angina. • ACE inhibitors: prevent formation of angiotensin II, which increases fluid volume and constriction of blood vessels. ACE inhibitors relax arterial walls and reduce fluid volume. They improve heart function and increase blood and oxygen flow to the heart, liver, and kidneys. They reduce risk of MI but not strokes. Side effects: dizziness, light-headedness, headache, dry nighttime cough, K buildup, and kidney problems. Monitor K levels and kidney function.
Hypertension
GENERAL CONSIDERATIONS
Classification of Hypertension by Blood Pressure
Classifications of Hypertension
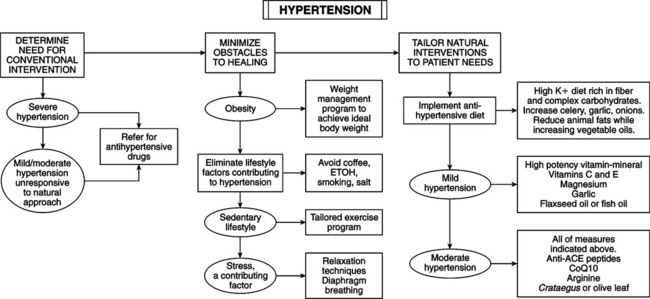
THERAPEUTIC CONSIDERATIONS
Conventional Antihypertensive Drugs
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Hypertension