4-6% of Caucasian adults > 50 years of age

• Recurrences common for both superficial and deep fibromatoses, but deaths only from deep fibromatoses

This fibromatosis is unusually superficial and arose in the chest wall of a young adult. These tumors are typically deep (deep fascia or within muscle).
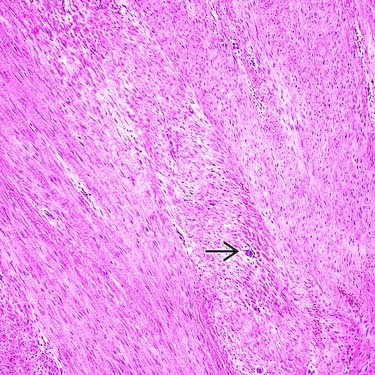
This image of a deep-type fibromatosis shows sweeping fascicles of spindle cells separated by regularly spaced collagen. Even at this magnification, small vessels are readily apparent
 .
.
This gross photograph shows a large, deep fibromatosis of the shoulder that has eroded into the scapula. Superficial portions of such lesions can be encountered on skin biopsies.
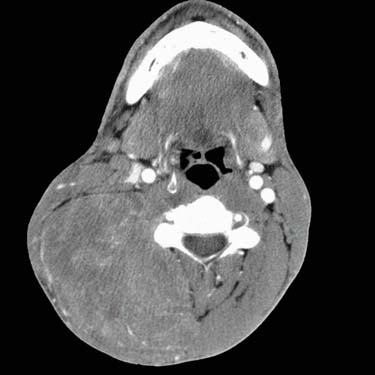
This radiologic image shows a large fibromatosis of the head and neck in an elderly alcoholic man. Although more arise in the shoulder girdles (or in the abdominal wall in young women), the head and neck is a common location for fibromatoses.
TERMINOLOGY
Synonyms
Definitions
• Palmar fibromatosis: Nodular myofibroblastic proliferation of volar surface of hand that is prone to local persistence but does not metastasize
• Plantar fibromatosis: Nodular myofibroblastic proliferation of plantar surface of foot that is prone to local persistence but does not metastasize
• Peyronie disease: Penile fibrous lesion causing various deformities; initially pain with erection, erectile dysfunction
• Knuckle pads: Well-circumscribed thickening of skin over metacarpophalangeal and, more commonly, proximal interphalangeal joints





Presentation

• Deep fibromatoses present as firm large masses, typically with intramuscular component
 Relationship to age and gender
Relationship to age and gender
Relationship to age and gender– In children and older adults, no gender predominance: Lesions of shoulders, chest wall, back, thigh, head, and neck




Treatment
• Superficial fibromatoses treated by excision




• Nonsurgical treatments for penile lesions: Verapamil, colchicine, Potaba, L-carnitine, and liposomal superoxide dismutase
• Deep fibromatoses treated by wide excision; for unresectable lesions, radiation, chemotherapy, hormone therapy

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
