(1)
Department of Pathology, Rutgers-New Jersey Medical School, Newark, NJ, USA
Keywords
Mesothelial hyperplasiaBenign multicystic mesotheliomaEndometriosisMalignancy arising in endometriosisEndosalpingiosisParaovarian/paratubal cystEctopic deciduaLeiomyoma of the broad ligamentFemale adnexal tumor of probably Wolffian origin (FATWO)Pseudomyxoma peritoneiSerous carcinomaPeritoneal malignant mesotheliomaAbdominal pregnancyDiffuse peritoneal leiomyomatosis10.1 Lesions of the Broad Ligament
Lesions arising in the broad ligament are uncommon, and most commonly endometriotic implants, leiomyomata, and hernias occurring through broad ligament defects. Rare broad ligament pregnancies have occurred (Table 10.1).
Table 10.1
Key points about broad ligament pathology
Most broad ligament lesions are leiomyomata or implants of endometriosis |
A variety of epithelial lesions arising elsewhere in the upper female genital tract can arise in the broad ligament as well |
Female Adnexal Tumor of Probable Wolffian Origin (FATWO) is a rare lesion that usually arises in the broad ligament |
10.1.1 Female Tumor of Probably Wolffian Origin (FATWO)
The most common site of origin of this rare neoplasm is the broad ligament, but they have also occurred in the ovary and retroperitoneum [1]. These lesions may be grossly cystic or solid and histologically have a variety of patterns, including solid, with characteristic sieve-like areas, and with a variety of cellular morphologic features (Fig. 10.1). The lesions stain for C-kit, which is helpful in establishing the diagnosis. Although most of these lesions behave in a benign manner, some have exhibited metastases, sometimes years later [1].
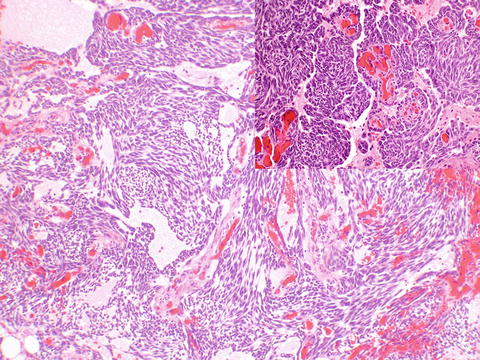
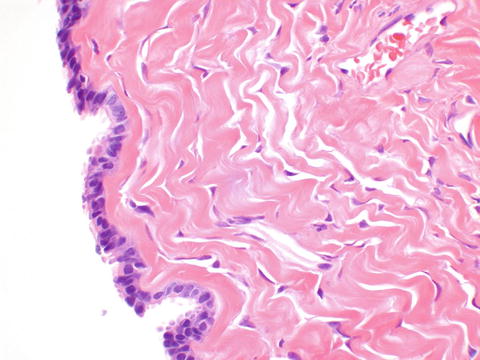
Fig. 10.1
Female adnexal tumor of probably Wolffian origin (FATWO) often shows a characteristic sieve-like pattern, but may appear more solid (inset, upper right)
10.1.2 Rare Broad Ligament Neoplasms and Broad Ligament Neoplasms More Often Occurring in Other Pelvic Locations
Epithelial neoplasms may occur in the broad ligament, including benign serous cystadenoma, as well as low malignant potential (“borderline”) serous neoplasms. Rare malignancies of various Müllerian epithelial types, sometimes in association with endometriosis, have been reported [1, 2]. A small number of cases of a papillary cystadenoma of mesonephric rather than Müllerian origin have been reported in association with von Hippel Lindau syndrome [3].
10.2 Lesions of the Peritoneum
A variety of sometimes histologically challenging lesions can affect the peritoneum. An index of suspicion, and sometimes immunohistochemistry, can be helpful in difficult cases (Table 10.2).
Table 10.2
Key points about peritoneal pathology
A variety of benign and malignant mesothelial proliferations may appear similar histologically and be difficult to distinguish. True invasion may be the only definitive histologic sign of malignancy |
Distinguishing papillary serous cystadenocarcinoma from peritoneal malignant mesothelioma usually requires an immunohistochemical panel of several antibodies |
Primary peritoneal high-grade serous carcinoma is thought to arise from serous tubal intraepithelial carcinoma and is diagnosed after tubal or ovarian primaries are ruled out |
Pseudomyxoma peritonei is most likely of primary appendiceal origin |
10.3 Benign Lesions of the Peritoneum
10.3.1 Endometriosis
Endometriosis involving peritoneum is often a clinical diagnosis and may not yield material for histopathological evaluation. Endometriosis often elicits a dense fibrotic response, particularly in omentum and abdominal wall (Fig. 10.2a). As in other sites, the histologic diagnosis requires endometrial glandular epithelium and stroma to confirm the diagnosis (Fig. 10.2b), which cannot be confirmed by hemosiderin-laden macrophages alone. A variety of Müllerian epithelial-derived malignancies (in particular clear cell adenocarcinoma and endometrioid adenocarcinoma) arising from pelvic soft tissues as well as ovary have arisen in association with endometriosis.
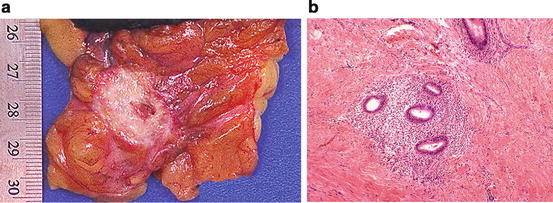
Fig. 10.2
Endometriosis. Endometriosis often provokes a dense fibrotic response around the hemorrhagic foci (a). Histologically, there are endometrial glands and stroma surrounded by dense fibroconnective tissue (b)
10.3.2 Endosalpingiosis
Endosalpingiosis is a common, clinically insignificant finding in peritoneum and pelvic and paraaortic lymph nodes and is comprised of small inclusions lined by a flattened or tubal-type epithelium (Fig. 10.3). Distinction from endometriosis is assisted by the lack of surrounding endometrial stroma in endosalpingiosis. Although endosalpingiosis may be an incidental finding in isolation, it is frequently associated with serous tumors of low malignant potential, and there may be some difficulties distinguishing endosalpingiosis from tumor implants histologically.
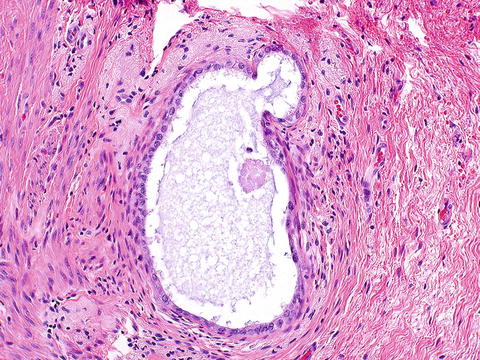
Fig. 10.3
Endosalpingiosis. There is a tubal epithelial type lining, and no cuff of endometrial stroma around the glandular space, distinguishing the lesion from endometriosis
10.3.3 Paraovarian/Paratubal Cyst
Paraovarian/paratubal cysts are usually benign thin-walled smooth serous lesions lined by a flat or tubal-type epithelium, although low malignant potential (“borderline”) and malignant neoplasms have occurred. These lesions may undergo torsion or present as a pelvic mass, or be asymptomatic. A histologic hallmark is in the wall of the benign tubal or flattened epithelial-lined cyst, which is composed of neither ovarian tissue nor tubal smooth muscle (Fig. 10.4). Most of these lesions are of Müllerian origin, but mesonephric (Wolffian) cysts can rarely occur [5].