Oxygen content as a function of hemoglobin. (With permission from Mulholland MW, Lillemoe KD, Doherty GM, Maier RV, Upchurch GR, eds. Greenfield’s Surgery. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.)
Oxygen Delivery
•Options to improve oxygen delivery include increasing hemoglobin, PaO2, SaO2, and stroke volume
•PaO2 = amount of unbound oxygen in arterial blood—measured by arterial blood gas
•SaO2 = amount of oxygen bound to hemoglobin—measured by pulse oximetry
•Oxygen delivery = arterial oxygen content (CaO2) × cardiac output (CO)
•CO = heart rate (HR) × stroke volume (SV)
•CaO2 = [(Hgb × 1.39) × SaO2] + [PaO2× 0.0031]
•1.39 = amount of oxygen in milliliter carried by each gram of fully oxygenated Hgb
•0.0031 = solubility of oxygen in plasma
•Oxygen delivery= {[(Hgb × 1.39) × SaO2] + [PaO2 × 0.0031]} × HR × SV
Increasing the hemoglobin in an anemic patient is usually the best way to improve oxygen delivery.
•Calculated as the difference between the arterial and venous oxygen content divided by the arterial oxygen content
•The pulmonary arteriole is the site of the lowest oxygen saturation in the body
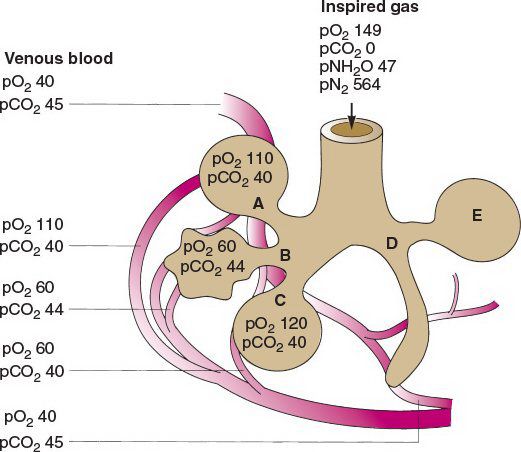
Variables affecting pulmonary gas exchange: (A) normal gas exchange, (B) hypoventilation, (C) decreased diffusion, (D) alveolar collapse, (E) shunting of blood flow away from normally ventilated alveolus. (With permission from Mulholland MW, Lillemoe KD, Doherty GM, Maier RV, Upchurch GR, eds. Greenfield’s Surgery. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.)
•Oxygen delivery:consumption ratio is 5:1
•Oxygen consumption is usually supply independent
•Oxygen consumption changes only when low levels of delivery are reached
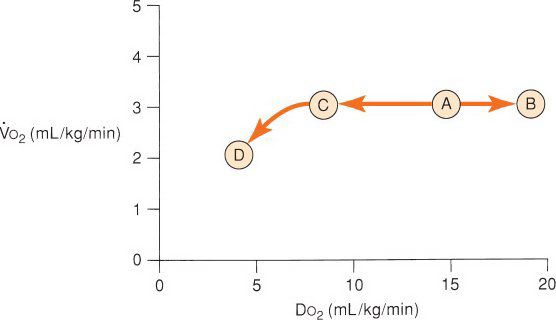
Oxygen consumption is supply independent except for very low oxygen delivery states. (With permission from Mulholland MW, Lillemoe KD, Doherty GM, Maier RV, Upchurch GR, eds. Greenfield’s Surgery. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.)
•SvO2—saturation of venous blood
•Normally is 65% to 75%
•Increased SvO2
•AV shunt
•Decreased oxygen extraction—sepsis, cirrhosis, cyanide toxicity, hyperthermia, paralysis, coma, sedation
•Hyperbaric O2
•Decreased SvO2
•Occurs with increased oxygen consumption or decreased delivery

Oxygen dissociation curve. The oxygen dissociation curve is shifted to the right with increased pCO2, acidity, 2,3-DPG (2,3-diphosphoglycerate), and temperature, thus favoring oxygen unloading to the tissues in times of physiologic stress. Bohr effect is a right shift with increased CO2.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


