• Immunostain for p16 is negative (there is no overexpression)
• In situ hybridization and PCR usually show presence of low-risk HPV (HPV 6 to 11)
Top Differential Diagnoses
• Verrucous carcinoma
• Warty carcinoma
• Papillomatosis of glans corona (pearly penile papules)
• Bowenoid papulosis
• Squamous cell carcinoma in situ or warty/basaloid penile intraepithelial neoplasia
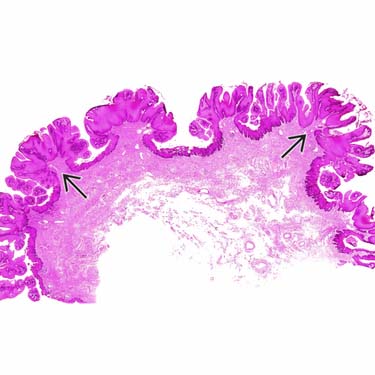
Low-Power View of Condyloma Acuminatum Condyloma acuminatum shows an exophytic papillomatous growth, regular and broad tumor base, and easily recognizable fibrovascular cores .
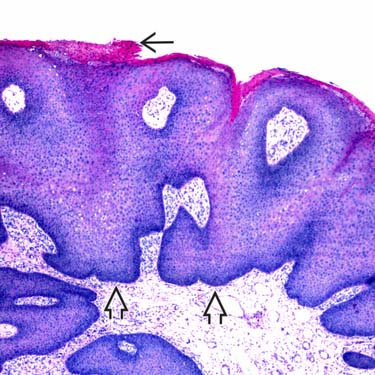
Prominent Koilocytosis in Condyloma Acuminatum Condyloma acuminatum is characterized by marked acanthosis, slight (as in this example) to marked papillomatosis, and a sharply demarcated, bulbous base . Note the focal parakeratosis .
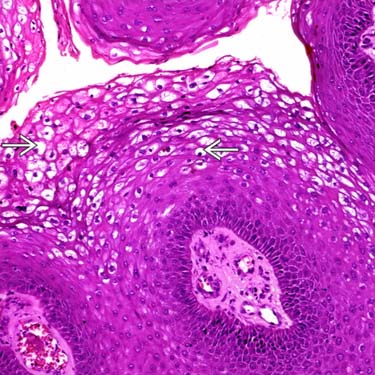
Higher Power View of Koilocytic Change Condyloma acuminatum is characterized by koilocytic change (nuclear wrinkling, a perinuclear halo , and often bi- and multinucleated nuclei). Koilocytosis tend to be confined to upper levels of the epithelium in contrast with warty carcinoma, where koilocytic change extends to deep infiltrative foci.
Binucleated Koilocytes in Condyloma Acuminatum Koilocytes have eosinophilic cytoplasm and are characterized by clear perinuclear halos and wrinkled and hyperchromatic nuclei. Binucleation is common .
TERMINOLOGY
Synonyms
• Genital wart
Definitions
• Exophytic and verruciform benign epithelial lesions
ETIOLOGY/PATHOGENESIS
Infectious Agents
• Caused by HPV
Low-risk serotypes 6 and 11 (90% of cases)
Other serotypes include 16, 18, 30-32, 42-44, 51-55
> 1 serotype may be found in lesion
CLINICAL ISSUES
Epidemiology
• Incidence
Very common STD
Penile lesions are more common in uncircumcised men than in circumcised ones
Topical treatment of vulvar dermatosis with corticosteroids and tacrolimus may reactivate old/latent lesions
Penile subclinical lesions appear to be more frequent in sexual partners of women with cervical intraepithelial neoplasia
• Age
Most frequent in young adults
– 2nd and 3rd decades of life
Uncommon in children
– Such cases should raise suspicion of sexual abuse
– HPV has been detected in young girls with lichen sclerosus without history of sexual abuse
– Spontaneous regression is common in children
~ 50% of cases
• Sex
Affect both sexes
Site
• Predilection for anogenital area
Males: Glans, prepuce, shaft
– May extend to meatus
Females: Labia minora, interlabial sulcus, area around introitus
– May extend into introitus
Both sexes: Perianal and more rarely oral cavity
Other less frequent locations: Abdomen, breast (nipple/areola)
Presentation
• Soft fleshy verruciform plaques
• Filiform lesions
• Lesion in coronal sulcus and vulva may be bulkier and macerated
• Flat (nearly macular lesions) may occur
• Tiny inconspicuous lesions may be difficult to detect
• Immunocompromised patients may show extensive lesions
Natural History
• Usually sexually transmitted
Spreads rapidly
• Variable incubation period
Usually 2-3 months
• Condylomas tend to recur
In ~ 30% of cases
May be due to persistence of HPV DNA in dermis &/or hair follicles
Treatment
• For small tumors: Cryosurgery, electrofulguration, laser ablation, and topical treatments
• For medium-sized and large tumors: Surgical excision
Prognosis
• Benign lesions
High recurrence rate (~ 30%)
Only gold members can continue reading. Log In or Register to continue


 .
.
 . Note the focal parakeratosis
. Note the focal parakeratosis  .
.
 , and often bi- and multinucleated nuclei). Koilocytosis tend to be confined to upper levels of the epithelium in contrast with warty carcinoma, where koilocytic change extends to deep infiltrative foci.
, and often bi- and multinucleated nuclei). Koilocytosis tend to be confined to upper levels of the epithelium in contrast with warty carcinoma, where koilocytic change extends to deep infiltrative foci.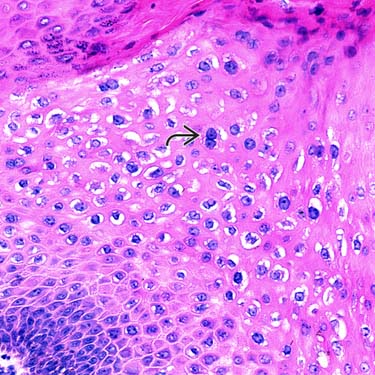
 .
.


 Topical treatment of vulvar dermatosis with corticosteroids and tacrolimus may reactivate old/latent lesions
Topical treatment of vulvar dermatosis with corticosteroids and tacrolimus may reactivate old/latent lesions


















