The cardiovascular system begins its activity when the fetus is barely 4 weeks old and is the last system to cease activity at the end of life. This body system is so vital that it helps define the presence of life.
The heart, arteries, veins, and lymphatics form the cardiovascular network that serves as the body’s transport system. This system brings life-supporting oxygen and nutrients to cells, removes metabolic waste products, and carries hormones from one part of the body to another.
The cardiovascular system, commonly called the circulatory system, may be divided into two branches: pulmonary and systemic circulations. In pulmonary circulation, blood picks up oxygen and liberates the waste product carbon dioxide. In systemic circulation (which includes coronary circulation), blood carries oxygen and nutrients to all active cells and transports waste products to the kidneys, liver, and skin for excretion.
Circulation requires normal heart function, which propels blood through the system by continuous rhythmic contractions. Blood circulates through three types of vessels: arteries, veins, and capillaries. The sturdy, pliable walls of the arteries adjust to the volume of blood leaving the heart. The aorta is the major artery arching out of the left ventricle; its segments and branches ultimately divide into minute, thinwalled (one cell thick) capillaries. Capillaries pass the blood to the veins, which return it to the heart. In the veins, valves prevent blood backflow.
Pathophysiologic changes
Pathophysiologic manifestations of cardiovascular disease may stem from aneurysm, cardiac shunts, embolus, release of cardiac enzymes and proteins, stenosis, thrombus, and valve incompetence.
ANEURYSM
An aneurysm is a localized outpouching or dilation of a weakened arterial wall. This weakness can be the result of either atherosclerotic plaque formation that erodes the vessel wall or the loss of elastin and collagen in the vessel wall. Congenital abnormalities in the media of the arterial wall, trauma, and infections, such as syphilis, may lead to aneurysm formation. A ruptured aneurysm may cause massive hemorrhage and death.
Several types of aneurysms can occur:
♦ A saccular aneurysm occurs when increased pressure in the artery pushes out a pouch on one side of the artery, creating a bulge. (See Types of aortic aneurysms.)
♦ A fusiform aneurysm develops when the arterial wall weakens around its circumference, creating a spindle-shaped aneurysm along an extended section.
♦ A dissecting aneurysm occurs when blood is forced between the layers of the arterial wall, causing them to separate and creating a false lumen.
♦ A false aneurysm develops when there’s a break in all layers of the arterial wall and blood leaks out — but is contained by surrounding structures—creating a pulsatile hematoma.
Types of aortic aneurysms
Common locations include:
♦ abdominal aortic aneurysm—an abnormal dilation in the arterial wall, generally occurring in the aorta between the renal arteries and iliac branches
♦ thoracic aortic aneurysm—an abnormal widening of the ascending, transverse, or descending part of the aorta
♦ cerebral aneurysm—a localized dilation of a cerebral artery that may arise at an arterial junction in the circle of Willis, the circular anastomosis forming the major cerebral arteries at the base of the brain
♦ femoral and popliteal aneurysms (sometimes called peripheral arterial aneurysms)—the end result of progressive atherosclerotic changes occurring in the walls (medial layer) of these major peripheral arteries.
CARDIAC SHUNTS
A cardiac shunt provides communication between the pulmonary and systemic circulations. Before birth, shunts between the right and left sides of the heart and between the aorta and pulmonary artery are a normal part of fetal circulation. After birth, however, the mixing of pulmonary and systemic blood or the movement of blood between the left and right sides of the heart is abnormal. Blood flows through a shunt from an area of high pressure to an area of low pressure or from an area of high resistance to an area of low resistance.
Left-to-right shunts
In a left-to-right shunt, blood flows from the left side of the heart to the right side through an atrial or ventricular defect, or from the aorta to the pulmonary circulation through a patent ductus arteriosus. Because the blood in the left side of the heart is rich in oxygen, a left-to-right shunt delivers oxygenated blood back to the right side of the heart or to the lungs. Consequently, a left-to-right shunt that occurs as a result of a congenital heart defect is called an acyanotic defect.
In a left-to-right shunt, pulmonary blood flow increases as blood is continually recirculated to the lungs, leading to hypertrophy of the pulmonary vessels. The increased amounts of blood circulated from the left side of the heart to the right side can result in right-sided heart failure. Eventually, left-sided heart failure may also occur.
Right-to-left shunts
A right-to-left shunt occurs when blood flows from the right side of the heart to the left side, such as in tetralogy of Fallot, or from the pulmonary artery directly into the systemic circulation through a patent ductus arteriosus. Because blood returning to the right side of the heart and the pulmonary artery is low in oxygen, a right-to-left shunt adds deoxygenated blood to the systemic circulation, causing hypoxia and cyanosis. A congenital defect that involves right-to-left shunts is therefore called a cyanotic defect. Common signs and symptoms of a right-to-left shunt related to poor tissue and organ perfusion include fatigue, increased respiratory rate, and clubbing of the fingers.
EMBOLUS
An embolus is a substance that circulates from one location in the body to another through the bloodstream. Although most emboli are blood clots from a thrombus, they may also consist of pieces of tissue, an air bubble, amniotic fluid, fat, bacteria, tumor cells, or a foreign substance.
Emboli that originate in the venous circulation, such as from deep vein thrombosis, travel to the right side of the heart to the pulmonary circulation and eventually lodge in a capillary, causing pulmonary infarction and even death. Most emboli in the arterial system originate from the left side of the heart from such conditions as arrhythmias, valvular heart disease, myocardial infarction, heart failure, or endocarditis. Arterial emboli may lodge in organs, such as the brain, kidneys, or extremities, causing ischemia or infarction.
RELEASE OF CARDIAC ENZYMES AND PROTEINS
When the heart muscle is damaged, the cell membrane’s integrity is impaired, and intracellular contents—including cardiac enzymes and proteins—are released and can be measured in the bloodstream. The release follows a characteristic rising and falling of values. The released enzymes include creatine kinase, lactate dehydrogenase, and aspartate aminotransferase; the proteins released include troponin T, troponin I, and myoglobin. (See Release of cardiac enzymes and proteins.)
STENOSIS
Stenosis is the narrowing of a tubular structure— for example, a blood vessel or heart valve. When an artery is stenosed, the tissues and organs perfused by that blood vessel may become ischemic, function abnormally, or die. An occluded vein may result in venous congestion and chronic venous insufficiency.
When a heart valve is stenosed, blood flow through that valve is reduced, causing blood to accumulate in the chamber behind the valve. Pressure in that chamber increases to pump against the resistance of the stenosed valve. Consequently, the heart has to work harder, resulting in hypertrophy. Hypertrophy and an increase in workload raise the heart’s oxygen demands. A heart with diseased coronary arteries may not be able to sufficiently increase oxygen supply to meet the increased demand.
When stenosis occurs in a valve on the left side of the heart, the increased pressure leads to greater pulmonary venous pressure and pulmonary congestion. As pulmonary vascular resistance rises, right-sided heart failure may occur. Stenosis in a valve on the right side of the heart causes an increase in pressures on the right side of the heart, leading to systemic venous congestion.
THROMBUS
A thrombus is a blood clot, consisting of platelets, fibrin, and red and white blood cells. It can form anywhere within the vascular system, including the arteries, veins, heart chambers, and heart valves.
Three conditions, known as Virchow’s triad, promote thrombus formation: endothelial injury, sluggish blood flow, and increased coagulability. When a blood vessel wall is injured, the endothelial lining attracts platelets and other inflammatory mediators, which may stimulate clot formation. Sluggish or abnormal blood flow also promotes thrombus formation by allowing platelets and clotting factors to accumulate and adhere to the blood vessel walls. Conditions that increase the coagulability of blood also promote clot formation.
The consequences of thrombus formation include occlusion of the blood vessel or the formation of an embolus (if a portion of a thrombus breaks loose and travels through the circulatory system until it lodges in a smaller vessel).
VALVE INCOMPETENCE
Valve incompetence, also called insufficiency or regurgitation, occurs when valve leaflets don’t completely close. Incompetence may affect valves of the veins or heart.
In the veins, valves keep the blood flowing in one direction, toward the heart. When valve leaflets close improperly, blood flows backward and pools above, causing that valve to weaken and become incompetent. Eventually, the veins become distended, which may result in varicose veins, chronic venous insufficiency, and venous stasis ulcers. Blood clots may form as blood flow becomes sluggish.
In the heart, incompetent valves allow blood to flow in both directions through the valve, increasing the volume of blood that must be pumped (as well as the heart’s workload) and resulting in hypertrophy. As blood volume in the heart increases, the involved heart chambers dilate to accommodate the increased volume. Although incompetence may occur in any heart valve, it’s more common in the mitral and aortic valves.
Release of cardiac enzymes and proteins
Because they’re released by damaged tissue, serum proteins and isoenzymes (catalytic proteins that vary in concentration in specific organs) can help identify the compromised organ and assess the extent of damage. After an acute myocardial infarction, cardiac enzyme and protein levels rise and fall in a characteristic pattern, as shown in the graph below.
Disorders
This section discusses disorders of the cardiovascular system, some of which are life-threatening. They include abdominal aortic aneurysm, acute coronary syndromes, arterial occlusive disease, atrial septal defect, Buerger’s disease, cardiac arrhythmias, cardiac tamponade, cardiomyopathy, coarctation of the aorta, coronary artery disease, endocarditis, heart failure, hypertension, myocarditis, patent ductus arteriosus, pericarditis, Raynaud’s disease, rheumatic fever and rheumatic heart disease, shock, tetralogy of Fallot, thrombophlebitis, transposition of the great arteries, valvular heart disease, varicose veins, and ventricular septal defect.
ABDOMINAL AORTIC ANEURYSM
Abdominal aortic aneurysm (AAA), an abnormal dilation in the arterial wall, generally occurs in the aorta between the renal arteries and iliac branches. Rupture, in which the aneurysm breaks open, resulting in profuse bleeding, is a common complication that occurs in larger aneurysms. Dissection occurs when the artery’s lining tears and blood leaks into the walls.
AAA is four times more common in men than in women and is most prevalent in whites who are between ages 40 and 70. Less than 50% of people with a ruptured AAA survive.
Causes
♦ Arteriosclerosis
♦ Blunt abdominal injury or Marfan syndrome (in children)
♦ Congenital weakening
♦ Cystic medial necrosis
♦ Hypertension
♦ Syphilis and other infections
♦ Trauma
Pathophysiology
Aortic aneurysms develop slowly. First, a focal weakness in the muscular layer of the aorta (tunica media), caused by degenerative changes, allows the inner layer (tunica intima) and outer layer (tunica adventitia) to stretch outward. Blood pressure within the aorta progressively weakens the vessel walls and enlarges the aneurysm.
Nearly all AAAs are fusiform, which causes the arterial walls to balloon on all sides. The resulting sac fills with necrotic debris and thrombi.
Signs and symptoms
Although AAAs usually don’t produce symptoms, most are evident (unless the patient is obese) as a pulsating mass in the periumbilical area, accompanied by a systolic bruit over the aorta. Other assessment findings may result from an enlarging or ruptured aneurysm, and may include:
♦ lumbar pain that radiates to the flank and groin from pressure on lumbar nerves (may signify enlargement and imminent rupture)
♦ diminished peripheral pulses or claudication if embolization occurs (rare)
♦ severe, persistent abdominal and back pain if the aneurysm ruptures into the peritoneal cavity
♦ weakness, sweating, tachycardia, and hypotension due to hemorrhage if the aneurysm ruptures.
Complications
♦ Rupture
♦ Obstruction of blood flow to other organs
♦ Embolization to a peripheral artery
♦ Diminished blood supply to vital organs resulting in organ failure (with rupture)
Diagnosis
Because AAAs seldom produce symptoms, they’re usually detected accidentally as the result of an X-ray or a routine physical examination. Several tests can confirm a suspected AAA:
♦ Serial ultrasound (sonography) can accurately determine the aneurysm’s size, shape, and location.
♦ Anteroposterior and lateral X-rays of the abdomen can detect aortic calcification, which outlines the mass, at least 75% of the time.
♦ Aortography shows the condition of vessels proximal and distal to the aneurysm and the aneurysm’s extent but may underestimate aneurysm diameter because it visualizes only the flow channel and not the surrounding clot.
♦ Computed tomography scan is used to diagnose and help determine the size of the aneurysm.
♦ Magnetic resonance imaging can be used as an alternative to aortography.
Treatment
♦ Conservative treatment when surgical repair carries a higher risk of mortality and in those patients for whom repair is unlikely to improve life expectancy
♦ Resection and replacement of damaged aortic section with Dacron or polytetrafluorethylene graft
♦ Surgical repair or replacement for symptomatic patients or those with aneurysms greater than 2″ (5 cm) in diameter
♦ Endoluminal stent grafting (not all patients with AAAs are candidates)
♦ Regular physical examination and ultrasound checks to detect enlargement
♦ External grafting (in patients with poor distal runoff)
♦ Control of hypercholesterolemia and hypertension
♦ A beta-adrenergic blocker to reduce the risk of aneurysm expansion and rupture
Special considerations
♦ AAAs require meticulous preoperative and postoperative care, psychological support, and comprehensive patient teaching. After diagnosis, if rupture isn’t imminent, elective surgery allows time for additional preoperative tests to evaluate the patient’s clinical status.
♦ Monitor vital signs, and type and crossmatch blood.
♦ Use only gentle abdominal palpation.
♦ As ordered, obtain renal function tests (blood urea nitrogen, creatinine, and electrolyte levels), blood samples (complete blood count with differential), electrocardiogram (ECG) and cardiac evaluation, baseline pulmonary function tests, and arterial blood gas (ABG) analysis.
Be alert for signs of rupture, which may be immediately fatal. Watch closely for signs of acute blood loss, such as decreasing blood pressure; increasing pulse and respiratory rate; cool, clammy skin; restlessness; and decreased sensorium.
If rupture occurs, get the patient to surgery immediately. A pneumatic antishock garment may be used while transporting him there. Surgery allows direct compression of the aorta to control hemorrhage. Large amounts of blood may be needed during the resuscitative period to replace blood loss. In such a patient, renal failure caused by ischemia is a major postoperative complication, possibly requiring hemodialysis.
♦ Before elective surgery, weigh the patient, insert an indwelling urinary catheter and an I.V. line, and assist with insertion of an arterial line and pulmonary artery catheter to monitor fluid and hemodynamic balance. Give a prophylactic antibiotic as ordered.
♦ Explain the surgical procedure and the expected postoperative care in the intensive care unit (ICU) for patients undergoing complex abdominal surgery (I.V. lines, endotracheal [ET] and nasogastric [NG] intubation, and mechanical ventilation).
♦ After surgery, in the ICU, closely monitor vital signs, intake and hourly output, neurologic status (level of consciousness, pupil size, and sensation in arms and legs), and ABG values. Assess the depth, rate, and character of respirations and breath sounds at least every hour.
♦ Watch for signs of bleeding (increased pulse and respiratory rates and hypotension) and back pain, which may indicate the graft is tearing. Check abdominal dressings for excessive bleeding or drainage. Be alert for temperature elevations and other signs of infection. After NG intubation for intestinal decompression, irrigate the tube frequently to ensure patency. Record the amount and type of drainage.
♦ Suction the ET tube often. If the patient can breathe unassisted and has good breath sounds and adequate ABG values, tidal volume, and vital capacity 24 hours after surgery, he’ll be extubated and require oxygen by mask.
♦ Weigh the patient daily to evaluate fluid balance.
♦ Help the patient walk as soon as he’s able (generally the second day after surgery).
♦ Provide psychological support for the patient and his family. Help ease their fears about the ICU, the threat of impending rupture, and surgery by providing appropriate explanations and answering all questions.
ACUTE CORONARY SYNDROMES
Acute myocardial infarction (MI), including ST-segment elevation MI (STEMI) and non-ST-segment elevation MI (NSTEMI), and unstable angina are now recognized as part of a group of clinical diseases called acute coronary syndromes (ACSs).
Rupture or erosion of plaque—an unstable and lipid-rich substance—initiates all coronary syndromes. The rupture results in platelet adhesions, fibrin clot formation, and activation of thrombin.
In cardiovascular disease—the leading cause of death in the United States and Western Europe—death usually results from cardiac damage after an MI. Each year, about 1 million people in the United States experience an MI. Incidence is higher in males younger than age 70. (Females have the protective effects of estrogen until menopause.) Mortality is high when treatment is delayed, and almost one-half of sudden deaths caused by an MI occur before hospitalization or within 1 hour of the onset of symptoms. The prognosis improves if vigorous treatment begins immediately.
Causes
Causes of ACS include atherosclerosis and embolus. In atherosclerosis, plaque (an unstable and lipidrich substance) forms and subsequently ruptures or erodes, resulting in platelet adhesions, fibrin clot formation, and activation of thrombin.
Risk factors for ACS include:
♦ diabetes
♦ family history of heart disease
♦ high-fat, high-carbohydrate diet
♦ hyperlipoproteinemia
♦ hypertension
♦ menopause
♦ obesity
♦ sedentary lifestyle
♦ smoking
♦ stress.
Pathophysiology
ACS most commonly results when a thrombus progresses and occludes blood flow. The degree of blockage and the time that the affected vessel remains occluded determine the type of infarct that occurs. The underlying effect is an imbalance in myocardial oxygen supply and demand. (See Stages of myocardial ischemia, injury, and infarct, page 130.)
For patients with unstable angina, a thrombus full of platelets partially occludes a coronary vessel. The partially occluded vessel may have distal microthrombi that cause necrosis in some myocytes. The smaller vessels infarct, thus placing the patient at higher risk for a NSTEMI.
Stages of myocardial ischemia, injury, and infarct
Three stages occur when there’s occlusion of a vessel: ischemia, injury, and infarct.
Ischemia
Ischemia is the first stage and indicates that blood flow and oxygen demand are out of balance. It can be resolved by improving flow or reducing oxygen needs. Electrocardiogram (ECG) changes reveal ST-segment depression or T-wave changes.
Injury
The second stage, injury, occurs when the ischemia is prolonged enough to damage the area of the heart. ECG changes usually reveal STsegment elevation (usually in two or more leads).
Infarct
Infarct is the the third stage and occurs with actual death of myocardial cells. Scar tissue eventually replaces the dead tissue, and the damage caused is irreversible.
In the earliest stage of a myocardial infarction (MI), hyperacute or very tall and narrow T waves may be seen on the ECG. Within hours the T waves become inverted and ST-segment elevation occurs in the leads facing the area of damage. The last change to occur in the evolution of an MI is the development of the pathologic Q wave, which is the only permanent ECG evidence of myocardial necrosis. Q waves are considered pathologic when they appear greater than or equal to 0.04 second wide and their height is greater than 25% of the R wave height in that lead. Pathologic Q waves develop in over 90% of the patients with ST-segment elevation MI. About 25% of the patients with a non-ST-segment elevation MI will develop pathologic Q waves and the remaining patients will have a non-Q wave MI.
If a thrombus fully occludes the vessel for a prolonged time, it’s classified as a STEMI. This type of an MI involves a greater concentration of thrombin and fibrin. (See How ACS affects the body.)
The location of the area of damage depends on the blood vessels involved:
How ACS affects the body
Acute coronary syndrome (ACS) can have farreaching effects and requires a multidisciplinary approach to care. Here’s what happens in ACS:
Cardiovascular system
♦ An area of viable ischemic tissue surrounds the zone of injury.
♦ When the heart muscle is damaged, the integrity of the cell membrane is impaired.
♦ Intracellular contents, including cardiac enzymes (such as creatine kinase, lactate dehydrogenase, and aspartate aminotransferase) and proteins (such as troponin T, troponin I, and myoglobin) are released.
♦ Within 24 hours, the infarcted area becomes edematous and cyanotic.
♦ During the next several days, leukocytes infiltrate the necrotic area and begin to remove necrotic cells, thinning the ventricular wall.
♦ Scar formation begins by the 3rd week after a myocardial infarction (MI); by the 6th week, scar tissue is well established.
♦ The scar tissue that forms on the necrotic area inhibits contractility.
♦ Compensatory mechanisms (vascular constriction, increased heart rate, and renal retention of sodium and water) try to maintain cardiac output.
♦ Ventricular dilation may also occur in a process called remodeling.
♦ Functionally, an MI may cause reduced contractility with abnormal wall motion, altered left ventricular compliance, reduced stroke volume, reduced ejection fraction, and elevated left ventricular end-diastolic pressure.
♦ Cardiogenic shock is caused by failure of the heart to perform as an effective pump and can result in low cardiac output, diminished peripheral perfusion, pulmonary congestion, and elevated systemic vascular resistance and pulmonary vascular pressures.
♦ Ineffective contractility of the heart leads to accumulation of blood in the venous circulation upstream to the failing ventricle.
♦ Arrhythmias can occur in the patient with an acute MI as a result of autonomic nervous system imbalance, electrolyte disturbances, ischemia, and slowed conduction in zones of ischemic myocardium.
Neurologic system
♦ Hypoperfusion of the brain results in altered mental status, involving changes in levels of consciousness, restlessness, irritability, confusion, or disorientation.
♦ Stupor or coma may result if the decrease in cerebral perfusion continues.
Renal system
♦ Shock and hypoperfusion from an MI cause the kidney to respond by conserving salt and water.
♦ Poor perfusion results in diminished renal blood flow, and increased afferent arteriolar resistance occurs, causing a decreased glomerular filtration rate.
♦ Increased amounts of antidiuretic hormone and aldosterone are released to help maintain perfusion. Urine formation, however, is reduced.
♦ Depletion of renal adenosine triphosphate stores results from prolonged renal hypoperfusion, causing impaired renal function.
Respiratory system
♦ Cardiogenic shock with left-sided heart failure results in increased fluid in the lungs. This process can overwhelm the capacity of the pulmonary lymphatics, resulting in interstitial and alveolar edema.
♦ Lung edema occurs when pulmonary capillary pressure exceeds 18 mm Hg.
♦ Pulmonary alveolar edema develops when pressures exceed 24 mm Hg, impairing oxygen diffusion.
♦ Increased interstitial and intra-alveolar fluid causes progressive reduction in lung compliance, increasing the work of ventilation and increasing perfusion of poorly ventilated alveoli.
Collaborative management
A cardiologist is consulted for initial assessment and treatment. A cardiothoracic surgeon may also be consulted if the patient requires invasive therapy. Other specialists may be required after initial therapy and treatment, such as a physical therapist for cardiac rehabilitation and a nutritionist for dietary and lifestyle changes.
♦ Anterior-wall MI—occurs when the left anterior descending artery becomes occluded.
♦ Septal-wall MI—typically accompanies an anterior-wall MI because the ventricular septum is supplied by the left anterior descending artery as well.
♦ Lateral-wall MI—caused by a blockage in the left circumflex artery, and usually accompanies an anterior- or inferior-wall MI.
♦ Inferior-wall MI—caused by occlusion of the right coronary artery; usually occurs alone or with a lateral-wall or right-ventricular MI.
♦ Posterior-wall MI— caused by occlusion of the right coronary artery or the left circumflex arteries.
♦ Right-ventricular MI—follows occlusion of the right coronary artery; this type of an MI rarely occurs alone (in 40% of patients, a rightventricular MI accompanies an inferior-wall MI).
Signs and symptoms
Signs and symptoms of ACS are caused by myocardial ischemia, resulting from an imbalance between supply and demand for myocardial oxygen.
These findings are typical of angina:
♦ burning, squeezing, and a crushing tightness in the substernal or precordial chest that may radiate to the left arm or shoulder blade, the neck, or the jaw
♦ pain after physical exertion, emotional excitement, exposure to cold, or consumption of a large meal.
Although other diagnoses may have chest pain as a symptom, retrosternal chest discomfort, pain, or pressure is a prime symptom of infarction. Patients typically describe these signs and symptoms of acute ischemia and an MI:
♦ uncomfortable pressure, squeezing, burning, severe persistent pain, or fullness in the center of the chest lasting several minutes (usually longer than 15 minutes)
♦ pain radiating to the shoulders, neck, arms, or jaw or pain in the back between the shoulder blades
♦ accompanying signs and symptoms of lightheadedness, fainting, sweating, nausea, shortness of breath, anxiety, or a feeling of impending doom.
Females may experience typical chest pain with acute ischemia and an MI; however, females—and occasionally males, elderly patients, and those patients with diabetes—may also experience atypical chest pain. Signs and symptoms include upper back discomfort between the shoulder blades, palpitations, a feeling of fullness in the neck, nausea, abdominal discomfort, dizziness, unexplained fatigue, and exhaustion or shortness of breath.
Complications
♦ Arrhythmias
♦ Ventricular irritability
♦ Heart failure
♦ Sudden death
Diagnosis
An electrocardiogram (ECG) helps to determine which area of the heart and which coronary arteries are involved. By recognizing danger early, you may be able to prevent an MI or even death. (See ECG characteristics in acute coronary syndromes.)
Other diagnostic tests may include:
♦ Serial cardiac enzyme and protein levels may show a characteristic rise and fall of cardiac enzymes, specifically CK-MB, the proteins troponin T and I, and myoglobin.
♦ Laboratory testing may reveal elevated white blood cell count and erythrocyte sedimentation rate and changes in electrolyte levels.
♦ Echocardiography may show ventricular wall motion abnormalities and may detect septal or papillary muscle rupture or identify pericardial effusions.
♦ Transesophageal echocardiography may reveal areas of decreased heart muscle wall movement, indicating ischemia.
♦ Chest X-rays may show left-sided heart failure, cardiomegaly, or other noncardiac causes of dyspnea or chest pain.
♦ Nuclear imaging scanning using thallium 201 and technetium 99 m can be used to identify areas of infarction and areas of viable muscle cells.
♦ Multiple-gated acquisition scanning is used to determine left ventricular function and identify aneurysms, problems with wall motion, and intracardiac shunting.
♦ Cardiac catheterization may be used to identify the involved coronary artery as well as to provide information on ventricular function and pressures and volumes within the heart.
Treatment
Treatment goals for patients experiencing ACS include:
♦ reducing the amount of myocardial necrosis in those with ongoing infarction
♦ decreasing cardiac workload and increasing oxygen supply to the myocardium
♦ preventing major adverse cardiac events
♦ providing for rapid defibrillation when ventricular fibrillation or pulseless ventricular tachycardia is present. (See Treating an MI,pages 134 and 135.)
ECG characteristics in acute coronary syndromes
The initial step in assessing a patient complaining of chest pain is to obtain an electrocardiogram (ECG). This should be done within 10 minutes of being seen by a physician. It’s crucial in determining the presence of myocardial ischemia, and the findings will direct the treatment plan.
Angina
Most patients with angina show ischemic changes on an ECG only during the attack. Because these changes may be fleeting, always obtain an order for and perform a 12-lead ECG as soon as the patient reports chest pain.
MI
According to the American Heart Association, patients should be classified as having STsegment elevation or new left bundle-branch block (LBBB), ST-segment depression or dynamic T-wave inversion, or nondiagnostic or normal ECG.
ST-segment elevation or new LBBB
♦ Patients with an ST-segment elevation greater than or equal to 1 mm in two or more contiguous leads or with new LBBB need to be treated for an acute MI.
♦ More than 90% of patients with this presentation will develop new Q waves and have positive serum cardiac markers.
♦ Repeating the ECG may be helpful for patients who present with hyperacute T waves.
ST-segment depression or dynamic T-wave inversion
♦ Patients with ST-segment depression indicating a posterior MI benefit most when an acute MI is diagnosed.
♦ Ischemia should be suspected with findings of ST-segment depression greater than or equal to 0.5 mm, marked symmetrical T-wave inversion in multiple precordial leads, and dynamic ST-T changes with pain.
♦ Patients who display persistent symptoms and recurrent ischemia, diffuse or widespread ECG abnormalities, heart failure, and positive serum markers are considered high risk.
Nondiagnostic or normal ECG
♦ A normal ECG won’t show ST-segment changes or arrhythmias.
♦ If the ECG is nondiagnostic, it may show an ST-segment depression of less than 0.5 mm or a T-wave inversion or flattening in leads with dominant R waves.
♦ Continue assessment of myocardial changes through use of serial ECGs, ST-segment monitoring, and serum cardiac markers.
♦ If further assessment is warranted, perform perfusion radionuclide imaging and stress echocardiography.
Initial treatment
Obtain a 12-lead ECG and serum cardiac markers to help confirm the diagnosis of an acute MI. Serum cardiac markers (especially troponin I and CK-MB) are used to distinguish unstable angina and NSTEMI.
Use the memory aid MONA, which stands for morphine, oxygen, nitroglycerin, and aspirin, to institute treatment of any patient experiencing ischemic chest pain or suspected ACS. Also, give:
♦ oxygen to increase oxygenation of blood
♦ nitroglycerin sublingually to relieve chest pain (unless systolic blood pressure is less than 90 mm Hg or heart rate is less than 50 beats/minute or greater than 100 beats/minute)
♦ morphine to relieve pain
♦ aspirin to inhibit platelet aggregation
♦ oral antiplatelet agent such as clopidogrel (Plavix) to help prevent clot formation.
For the patient with unstable angina and NSTEMI, treatment includes the above initial measures as well as:
♦ a beta-adrenergic blocker to reduce the heart’s workload and oxygen demands
♦ heparin and a glycoprotein IIb/IIIa inhibitor to minimize platelet aggregation and the danger of coronary occlusion with high-risk patients (patients with planned cardiac catheterization and positive troponin)
♦ nitroglycerin I.V. to dilate coronary arteries and relieve chest pain (unless systolic blood pressure is less than 90 mm Hg or heart rate is less than 50 beats/minute or more than 100 beats/minute)
♦ an antiarrhythmic, transcutaneous pacing (or transvenous pacemaker), or defibrillation, if the patient has ventricular fibrillation or pulseless ventricular tachycardia (VT)
♦ percutaneous coronary interventions (PCI) or coronary artery bypass graft surgery for obstructive lesions
This flowchart shows how treatments can be applied to a myocardial infarction (MI) at various stages of its development.
♦ an antilipemic to reduce elevated serum cholesterol or triglyceride levels.
For the patient with STEMI, treatment includes the above initial measures and these additional measures:
♦ thrombolytic therapy (unless contraindicated) within 12 hours of onset of symptoms to restore vessel patency and minimize necrosis in STEMI
♦ I.V. heparin to promote patency in the affected coronary artery
♦ a beta-adrenergic blocker to reduce myocardial workload
♦ a glycoprotein IIb/IIIa inhibitor to reduce platelet aggregation
♦ an antiarrhythmic, transcutaneous pacing (or transvenous pacemaker), or defibrillation, if the patient has ventricular fibrillation or pulseless VT
♦ an angiotensin-converting enzyme (ACE) inhibitor to reduce afterload and preload and prevent remodeling (begin in STEMI 6 hours after admission or when the patient’s condition is stable)
♦ interventional procedures (such as PCI, stent placement, or surgical procedures, such as coronary artery bypass graft) may open blocked or narrowed arteries.
Special considerations
Care for patients who have suffered an MI is directed toward detecting complications, preventing further myocardial damage, and promoting comfort, rest, and emotional well-being. Most MI patients receive treatment in the intensive care unit (ICU), where they’re under constant observation for complications.
♦ On admission to the ICU, monitor and record the patient’s ECG, blood pressure, temperature, and heart and breath sounds.
♦ Assess and record the severity and duration of pain, and administer an analgesic. Avoid I.M. injections; absorption from the muscle is unpredictable and bleeding is likely if the patient is receiving thrombolytic therapy.
♦ Check the patient’s blood pressure after giving nitroglycerin, especially the first dose.
♦ Frequently monitor the ECG to detect rate changes or arrhythmias. Place rhythm strips in the patient’s chart periodically for evaluation.
♦ During episodes of chest pain, obtain a 12-lead ECG (before and after nitroglycerin therapy as well), blood pressure, and pulmonary artery catheter measurements and monitor them for changes.
♦ Watch for signs and symptoms of fluid retention (crackles, cough, tachypnea, and edema), which may indicate impending heart failure. Carefully monitor daily weight, intake and output, respirations, serum enzyme levels, and blood pressure. Auscultate for adventitious breath sounds periodically (patients on bed rest commonly have atelectatic crackles, which disappear after coughing), for S3 or S4 gallops, and for new-onset heart murmurs.
♦ Organize patient care and activities to maximize periods of uninterrupted rest.
♦ Initiate a cardiac rehabilitation program, which typically includes education regarding heart disease, exercise, and emotional support for the patient and his family.
♦ Ask the dietary department to provide a clear liquid diet until nausea subsides. A lowcholesterol, low-sodium, low-fat, high-fiber diet may be prescribed.
♦ Provide a stool softener to prevent straining during defecation, which causes vagal stimulation and may slow the heart rate. Allow use of a bedside commode, and provide as much privacy as possible.
♦ Assist with range-of-motion exercises. If the patient is completely immobilized by a severe MI, turn him often. Antiembolism stockings help prevent venostasis and thrombophlebitis.
♦ Provide emotional support and help reduce stress and anxiety; administer a tranquilizer as needed. Explain procedures and answer questions. Explaining the ICU environment and routine can ease anxiety. Involve the patient’s family in his care as much as possible.
Preparing for discharge
♦ Thoroughly explain dosages and therapy to promote compliance with the prescribed drug regimen and other treatment measures. Warn about drug adverse effects, and advise the patient to watch for and report signs and symptoms of toxicity (anorexia, nausea, vomiting, and yellow vision, for example, if the patient is receiving digoxin).
♦ Review dietary restrictions with the patient. If he must follow a low-sodium or a low-fat, low-cholesterol diet, provide a list of foods that he should avoid. Ask the dietitian to speak to the patient and his family.
♦ Counsel the patient to resume sexual activity progressively.
♦ Advise the patient to report typical or atypical chest pain. Postinfarction syndrome may develop, producing chest pain that must be differentiated from a recurrent MI, a pulmonary infarct, or heart failure.
♦ If the patient has a Holter monitor in place, explain its purpose and use.
♦ Stress the need to stop smoking.
♦ Encourage participation in a cardiac rehabilitation program.
♦ Review follow-up procedures, such as office visits and treadmill testing, with the patient.
ARTERIAL OCCLUSIVE DISEASE
Arterial occlusive disease, also called peripheral artery disease, is the obstruction or narrowing of the lumen of the aorta and its major branches, causing an interruption of blood flow, usually to the legs and feet. This disorder may affect the carotid, vertebral, innominate, subclavian, mesenteric, iliac, and femoral arteries.
Arterial occlusive disease is more common in males than in females. The prognosis depends on the occlusion’s location, the development of collateral circulation to counteract reduced blood flow and, in acute disease, the time elapsed between occlusion and its removal.
Causes
Arterial occlusive disease is a common complication of atherosclerosis. The occlusive mechanism may be endogenous, due to emboli formation or thrombosis, or exogenous, due to trauma or fracture.
Other predisposing factors include:
♦ aging
♦ diabetes
♦ family history of vascular disorders, an MI, or a stroke
♦ hyperlipidemia
♦ hypertension
♦ smoking.
Pathophysiology
Arterial occlusive disease is almost always the result of atherosclerosis, in which fatty, fibrous plaques narrow the lumen of blood vessels. This occlusion can occur acutely or progressively over 20 to 40 years, with areas of vessel branching, or bifurcation, being the most common sites. The narrowing of the lumens reduces the blood volume that can flow through them, causing arterial insufficiency to the affected area. Ischemia usually occurs after the vessel lumens have narrowed by at least 50%, reducing blood flow to a level at which it no longer meets the needs of tissue and nerves.
Aging causes sclerotic changes in blood vessels, which leads to decreased elasticity and narrowing of the lumen, further contributing to the development of arterial occlusive disease. In people older than age 70, the prevalence of the disease is estimated to be 10% to 18%.
Signs and symptoms
Signs and symptoms of arterial occlusive disease depend on the site of the occlusion. (See Types of arterial occlusive disease,page 138.)
Complications
♦ Severe ischemia and necrosis
♦ Skin ulceration
♦ Gangrene, which can lead to limb amputation
♦ Impaired nail and hair growth
♦ Stroke or transient ischemic attack
♦ Peripheral or systemic embolism
Diagnosis
Diagnosis of arterial occlusive disease is usually indicated by patient history and physical examination. These pertinent tests support the diagnosis:
♦ Arteriography demonstrates the type (thrombus or embolus), location, and degree of obstruction and the collateral circulation. Arteriography is particularly useful in chronic disease or for evaluating candidates for reconstructive surgery.
♦ Doppler ultrasonography and plethysmography are noninvasive tests that show decreased blood flow distal to the occlusion in acute disease.
♦ Ankle-branchial index (ABI) (the ratio of systolic blood pressure at the ankle to that at the arm) decreases with worsening arterial occlusive disease. An ABI less than 0.9 indicates some degree of arterial occlusive disease.
♦ Ophthalmodynamometry helps determine the degree of obstruction in the internal carotid artery by comparing ophthalmic artery pressure to brachial artery pressure on the affected side. More than a 20% difference between pressures suggests insufficiency.
♦ EEG and computed tomography scan may be necessary to rule out brain lesions.
Treatment
Treatment of arterial occlusive disease depends on the cause, location, and size of the obstruction. For mild chronic disease, supportive measures include smoking cessation, hypertension control, hyperlipidemia control, and mild exercise, such as walking. For carotid artery occlusion, the patient should begin life-long aspirin therapy. For chronic occlusive disease, antiplatelet therapy should begin with aspirin (first-line agent), clopidogrel, or ticlopidine. Cilostazol is recommended for patients with disabling intermittent claudication who are poor candidates for surgery.
Acute arterial occlusive disease usually requires immediate anticoagulation therapy with heparin and surgery to restore circulation to the affected area, for example:
♦ Embolectomy—A balloon-tipped Fogarty catheter is used to remove thrombotic material from the artery. Embolectomy is used mainly for mesenteric, femoral, or popliteal artery occlusion.
Types of arterial occlusive disease
Site of occlusion
Signs and symptoms
Carotid arterial system
♦ Internal carotids
♦ External carotids
Neurologic dysfunction: transient ischemic attacks (TIAs) due to reduced cerebral circulation produce unilateral sensory or motor dysfunction (transient monocular blindness, hemiparesis), possible aphasia or dysarthria, confusion, decreased mentation, and headache; recurrent clinical features usually lasting 5 to 10 minutes, but may persist up to 24 hours and may herald a stroke; absent or decreased pulsation with an auscultatory bruit over the affected vessels
Vertebrobasilar system
♦ Vertebral arteries
♦ Basilar arteries
Neurologic dysfunction: TIAs of brain stem and cerebellum produce binocular visual disturbances, vertigo, dysarthria, and “drop attacks” (falling down without loss of consciousness); less common than carotid TIA
Innominate artery
Neurologic dysfunction: signs and symptoms of vertebrobasilar occlusion; indications of ischemia (claudication) of right arm; possible bruit over right side of neck
Subclavian artery
Subclavian steal syndrome (characterized by blood backflow from the brain through the vertebral artery on the same side as the occlusion, into the subclavian artery distal to the occlusion); clinical effects of vertebrobasilar occlusion and exercise-induced arm claudication; possible gangrene, usually limited to the digits
Mesenteric artery
♦ Superior (most commonly affected)
♦ Celiac axis
♦ Inferior
Bowel ischemia, infarct necrosis, and gangrene; sudden, acute abdominal pain; nausea and vomiting; diarrhea; leukocytosis; and shock due to massive intraluminal fluid and plasma loss
Aortic bifurcation
(saddle-block occlusion, a medical emergency associated with cardiac embolization)
Sensory and motor deficits (muscle weakness, numbness, paresthesia, paralysis) and signs and symptoms of ischemia (sudden pain; cold, pale legs with decreased or absent peripheral pulses) in both legs
Iliac artery
(Leriche’s syndrome)
Intermittent claudication of lower back, buttocks, and thighs, relieved by rest; absent or reduced femoral or distal pulses; possible bruit over femoral arteries; impotence in males
Femoral and popliteal arteries
(associated with aneurysm formation)
Intermittent claudication of the calves on exertion; ischemic pain in feet; pretrophic pain (heralds necrosis and ulceration); leg pallor and coolness; blanching of feet on elevation; gangrene; no palpable pulses in ankles and feet
♦ Thromboendarterectomy—Opening of the occluded artery and direct removal of the obstructing thrombus and the medial layer of the arterial wall; usually performed after angiography and commonly used with autogenous vein or Dacron bypass surgery (femoral-popliteal or aortofemoral).
♦ Patch grafting—The thrombosed arterial segment is removed and replaced with an autogenous vein or Dacron graft.
♦ Bypass graft—Blood flow is diverted through an anastomosed autogenous or Dacron graft past the thrombosed segment.
♦ Thrombolytic therapy—Urokinase, streptokinase, or alteplase causes lysis of clot around or in the plaque.
♦ Atherectomy—Plaque is excised using a drill or slicing mechanism.
♦ Balloon angioplasty—Balloon inflation compresses the obstruction.
♦ Laser angioplasty—Obstruction is excised and vaporized using hot-tip lasers.
♦ Stents—A mesh of wires that stretch and mold to the arterial wall is inserted to prevent reocclusion. This new adjunct follows laser angioplasty or atherectomy.
Combined therapy, which is simply the concomitant use of any surgical treatment listed above, may be appropriate. Also, lumbar sympathectomy is a possible adjunct to surgery, depending on the condition of the sympathetic nervous system.
Amputation becomes necessary if arterial reconstructive surgery fails or if gangrene, persistent infection, or intractable pain develops. Other therapy may include bowel resection after restoration of blood flow (for mesenteric artery occlusion).
Special considerations
♦ Provide comprehensive patient teaching, such as proper foot care.
♦ Explain all diagnostic tests and procedures.
♦ Advise the patient to stop smoking and to follow the prescribed medical regimen.
Preoperatively
During an acute episode:
♦ Assess the patient’s circulatory status by checking for the most distal pulses and by inspecting his skin color and temperature.
♦ Provide pain relief as needed.
♦ Administer heparin by continuous I.V. drip, as ordered, using an infusion pump to ensure the proper flow rate.
♦ Wrap the patient’s affected foot in soft cotton batting, and reposition it frequently to prevent pressure on any one area.
♦ Strictly avoid elevating or applying heat to the affected leg.
♦ Watch for signs of fluid and electrolyte imbalance, and monitor intake and output for signs of renal failure (urine output less than 30 ml/hour).
♦ If the patient has carotid, innominate, vertebral, or subclavian artery occlusion, monitor him for signs and symptoms of stroke, such as numbness in his arm or leg and intermittent blindness.
Postoperatively
During postoperative management:
♦ Monitor the patient’s vital signs. Continuously assess his circulatory function by inspecting skin color and temperature and by checking for distal pulses. In charting, compare earlier assessments and observations. Watch closely for signs of hemorrhage (tachycardia and hypotension), and check dressings for excessive bleeding.
♦ In carotid, innominate, vertebral, or subclavian artery occlusion, assess the patient’s neurologic status frequently for changes in level of consciousness or muscle strength and pupil size.
♦ In mesenteric artery occlusion, connect a nasogastric tube to low intermittent suction. Monitor the patient’s intake and output (low urine output may indicate damage to renal arteries during surgery). Check bowel sounds for return of peristalsis. Increased abdominal distention and tenderness may indicate extension of bowel ischemia with resulting gangrene, necessitating further excision, or it may indicate peritonitis.
♦ In saddle block occlusion, check distal pulses for adequate circulation. Watch for signs of renal failure and mesenteric artery occlusion (severe abdominal pain) as well as cardiac arrhythmias, which may precipitate embolus formation.
♦ In iliac artery occlusion, monitor urine output for signs of renal failure from decreased perfusion to the kidneys as a result of surgery. Provide meticulous catheter care.
♦ In femoral and popliteal artery occlusions, assist the patient with early ambulation, but discourage prolonged sitting.
♦ After amputation, check the patient’s stump carefully for drainage and record its color and amount and the time. Elevate the stump, as ordered, and administer an adequate amount of analgesic. Because phantom limb pain is common, explain this phenomenon to the patient.
♦ When preparing the patient for discharge, instruct him to watch for signs and symptoms of recurrence (pain, pallor, numbness, paralysis, and absence of pulse), which can result from graft occlusion or occlusion at another site. Warn him against wearing constrictive clothing.
ATRIAL SEPTAL DEFECT
In atrial septal defect (ASD)—a congenital heart defect that increases pulmonary blood flow—an opening between the left and right atria allows blood to flow from left to right, resulting in ineffective pumping of the heart, thus increasing the risk of heart failure.
The three types of ASDs include:
♦ an ostium secundum defect, the most common type, which occurs in the region of the fossa ovalis and, occasionally, extends inferiorly, close to the vena cava
♦ a sinus venosus defect, which occurs in the superior-posterior portion of the atrial septum, sometimes extending into the vena cava, and is almost always associated with abnormal drainage of pulmonary veins into the right atrium
♦ an ostium primum defect, which occurs in the inferior portion of the septum primum and is usually associated with atrioventricular valve abnormalities (cleft mitral valve) and conduction defects.
ASD accounts for about 10% of congenital heart defects and is almost twice as common in females as in males, with a strong familial tendency. Although an ASD is usually a benign defect during infancy and childhood, delayed development of symptoms and complications makes it one of the most common congenital heart defects diagnosed in adults.
The prognosis is excellent in asymptomatic patients and in those with uncomplicated surgical repair, but poor in patients with cyanosis caused by large, untreated defects.
Causes
♦ Unknown
♦ Ostium primum defects commonly occurring in patients with Down syndrome
Pathophysiology
In an ASD, blood shunts from the left atrium to the right atrium because the left atrial pressure is normally slightly higher than the right atrial pressure. This pressure difference forces large amounts of blood through a defect. This shunt results in right heart volume overload, affecting the right atrium, right ventricle, and pulmonary arteries. Eventually, the right atrium enlarges, and the right ventricle dilates to accommodate the increased blood volume. If pulmonary artery hypertension develops, increased pulmonary vascular resistance and right ventricular hypertrophy follow. In some adults, irreversible pulmonary artery hypertension causes reversal of the shunt direction, which results in unoxygenated blood entering the systemic circulation, causing cyanosis.
Signs and symptoms
♦ Fatigue after exertion caused by decreased cardiac output from the left ventricle
♦ Early systolic to midsystolic murmur at the second or third left intercostal space, caused by extra blood passing through the pulmonic valve
♦ Low-pitched diastolic murmur at the lower left sternal border, more pronounced on inspiration, resulting from increased tricuspid valve flow in patients with large shunts
♦ Fixed, widely split S2 due to delayed closure of the pulmonic valve, resulting from an increased volume of blood
♦ Systolic click or late systolic murmur at the apex, resulting from mitral valve prolapse in older children with an ASD
♦ Clubbing and cyanosis, if a right-to-left shunt develops
An infant may be cyanotic because he has a cardiac or pulmonary disorder. Cyanosis that worsens with crying is most likely associated with cardiac causes because crying increases pulmonary resistance to blood flow, resulting in an increased right-to-left shunt. Cyanosis that improves with crying is most likely associated with pulmonary causes because deep breathing improves tidal volume.
Complications
♦ Physical underdevelopment
♦ Respiratory tract infections
♦ Heart failure
♦ Atrial arrhythmias
♦ Mitral valve prolapse
Diagnosis
A history of increasing fatigue and characteristic physical features suggest an ASD. These tests confirm the diagnosis:
♦ Chest X-ray shows an enlarged right atrium and right ventricle, a prominent pulmonary artery, and increased pulmonary vascular markings.
♦ Electrocardiography results may be normal, but they commonly show right-axis deviation, a prolonged PR interval, varying degrees of right bundle-branch block, right ventricular hypertrophy, atrial fibrillation (particularly in severe cases in patients older than age 30) and, in ostium primum defect, left-axis deviation.
♦ Echocardiography measures right ventricular enlargement, may locate the defect, and shows volume overload in the right side of the heart. It may reveal right ventricular and pulmonary artery dilation.
♦ Two-dimensional echocardiography with color Doppler flow, contrast echocardiography, or both have supplanted cardiac catheterization as the confirming tests for an ASD. Cardiac catheterization is used if inconsistencies exist in the clinical data or if significant pulmonary hypertension is suspected.
Treatment
Operative repair is advised for the patient with an uncomplicated ASD with evidence of significant left-to-right shunting. Ideally, this is performed when the patient is between ages 2 and 4.
Operative treatment shouldn’t be performed on a patient with small defects and trivial left-toright shunts. Because an ASD seldom produces complications in an infant or a toddler, surgery can be delayed until preschool or early school age. A large defect may need immediate surgical closure with sutures or a patch graft. Alternatively, placement of a wire mesh septal occluder device during cardiac catheterization is becoming a more common intervention than open-heart surgery. Patients recover more quickly from this procedure than from surgery.
Special considerations
♦ Before cardiac catheterization, explain pretest and posttest procedures to the child and parents. If possible, use drawings or other visual aids to explain it to the child.
♦ As needed, teach the patient about antibiotic prophylaxis to prevent infective endocarditis.
♦ If surgery is scheduled, teach the child and parents about the intensive care unit and introduce them to the staff. Show parents where they can wait during the operation. Explain postoperative procedures, tubes, dressings, and monitoring equipment.
♦ After surgery, closely monitor the patient’s vital signs, central venous and intra-arterial pressures, and intake and output. Watch for atrial arrhythmias, which may remain uncorrected.
BUERGER’S DISEASE
Buerger’s disease (sometimes called thromboangiitis obliterans)—an inflammatory, nonatheromatous occlusive condition—impairs circulation to the legs, feet and, occasionally, hands. It affects 6 out of every 10,000 people, most commonly occuring in men ages 20 to 40 who have a history of smoking or chewing tobacco.
Causes
♦ Unknown
♦ Definite link to smoking has been found, suggesting a hypersensitivity reaction to nicotine
Pathophysiology
In Buerger’s disease, polymorphonuclear leukocytes infiltrate the walls of small and mediumsized arteries and veins. Thrombus develops in the vascular lumen, eventually occluding and obliterating portions of the small vessels, resulting in decreased blood flow to the feet and legs. This diminished blood flow may produce ulceration and, eventually, gangrene.
Signs and symptoms
♦ Intermittent claudication of the instep, which is aggravated by exercise and relieved by rest, resulting from tissue ischemia
♦ Initially, coldness, cyanosis, and numbness in feet during exposure to low temperature, resulting from diminished blood flow; later, redness, heat, and tingling
♦ Impaired peripheral pulses and migratory superficial thrombophlebitis caused by inflammatory changes in the vessel walls
Complications
♦ Ulceration, muscle atrophy, and gangrene due to impaired blood flow
♦ Painful fingertip ulcerations if the hands are affected
Diagnosis
Patient history and physical examination strongly suggest Buerger’s disease. Supportive diagnostic tests include:
♦ Doppler ultrasonography to show diminished circulation in the peripheral vessels
♦ plethysmography to help detect decreased circulation in the peripheral vessels
♦ arteriography to locate lesions and rule out atherosclerosis.
Treatment
The primary goals of treatment are to relieve symptoms and prevent complications. Such therapy may include:
♦ an exercise program that uses gravity to fill and drain the blood vessels
♦ in severe disease, a lumbar sympathectomy to increase blood supply to the skin
♦ possibly amputation for nonhealing ulcers, intractable pain, or gangrene.
Special considerations
♦ Strongly urge the patient to permanently discontinue smoking to enhance the effectiveness of treatment. If necessary, refer him to a self-help group to stop smoking.
♦ Warn the patient to avoid such precipitating factors as emotional stress, exposure to extreme temperatures, and trauma.
♦ Teach proper foot care, especially the importance of wearing well-fitting shoes and cotton or wool socks. Show the patient how to inspect his feet daily for cuts, abrasions, and signs of skin breakdown, such as redness and soreness. Remind him to seek medical attention at once after trauma.
♦ If the patient has ulcers and gangrene, enforce bed rest and use a padded footboard or bed cradle to prevent pressure from bed linens. Protect the feet with soft padding. Wash them gently with a mild soap and tepid water, rinse thoroughly, and pat dry with a soft towel.
♦ Provide emotional support. If necessary, refer the patient for psychological counseling to help him cope with restrictions imposed by this chronic disease. If he has undergone amputation, assess rehabilitative needs, especially regarding changes in body image. Refer him to a physical therapist, an occupational therapist, or a social service agency, as needed.
CARDIAC ARRHYTHMIAS
In arrhythmias, abnormal electrical conduction or automaticity changes the heart’s rate and rhythm. Arrhythmias vary in severity, from those that are mild, asymptomatic, and require no treatment (such as sinus arrhythmia, in which heart rate increases and decreases with respiration) to catastrophic ventricular fibrillation, which requires immediate resuscitation. Arrhythmias are generally classified according to their origin (ventricular or supraventricular). Their effect on cardiac output and blood pressure, partially influenced by the site of origin, determines their clinical significance.
Causes
♦ Acid-base imbalances
♦ Cellular hypoxia
♦ Congenital defects
♦ Connective tissue disorders
♦ Degeneration of the conductive tissue
♦ Drug toxicity
♦ Electrolyte imbalances
♦ Emotional stress
♦ Hypertrophy of the heart muscle
♦ Myocardial ischemia or infarction
♦ Organic heart disease
Keep in mind that each arrhythmia may have its own specific causes. (See Types of cardiac arrhythmias, pages 144,145,146,147,148,149,150,151.)
Pathophysiology
Arrhythmias may result from enhanced automaticity, reentry, escape beats, or abnormal electrical conduction. (See Comparing normal and abnormal conduction,pages 150 and 151.)
Signs and symptoms
Signs and symptoms of arrhythmias result from reduced cardiac output and altered perfusion to the organs, and may include:
♦ dyspnea
♦ hypotension
♦ dizziness, syncope, and weakness
♦ chest pain
♦ cool, clammy skin
♦ altered level of consciousness
♦ reduced urine output.
Complications
♦ Sudden cardiac death
♦ Myocardial infarction
♦ Heart failure
♦ Thromboembolism
Diagnosis
♦ Electrocardiography detects arrhythmias as well as ischemia and infarction that may result in arrhythmias.
♦ Laboratory testing may reveal electrolyte abnormalities, acid-base abnormalities, or drug toxicities that may cause arrhythmias.
♦ Holter monitoring, event monitoring, and loop recording can detect arrhythmias and the effectiveness of drug therapy during a patient’s daily activities.
♦ Exercise testing may detect exercise-induced arrhythmias.
♦ Electrophysiologic testing identifies the mechanism of an arrhythmia and the location of accessory pathways; it also assesses the effectiveness of antiarrhythmics, radiofrequency ablation, and implanted cardioverter-defibrillators.
Treatment
Follow the specific treatment guidelines for each arrhythmia. (See Types of cardiac arrhythmias, pages 144,145,146,147,148,149,150,151.)
Special considerations
♦ Assess an unmonitored patient for rhythm disturbances.
♦ If the patient’s pulse is abnormally rapid, slow, or irregular, watch for signs of hypoperfusion, such as hypotension and diminished urine output.
♦ Document arrhythmias in a monitored patient, and assess him for possible causes and effects.
♦ When life-threatening arrhythmias develop, rapidly assess level of consciousness, respirations, and pulse rate.
♦ Initiate cardiopulmonary resuscitation, if indicated.
♦ Evaluate the patient for altered cardiac output resulting from arrhythmias.
♦ Administer medications as ordered, and prepare to assist with medical procedures, if indicated (for example, cardioversion).
♦ Monitor the patient for predisposing factors— such as fluid and electrolyte imbalances—and signs of drug toxicity, especially with digoxin. If you suspect drug toxicity, report such signs to the physician immediately and withhold the next dose.
♦ To prevent arrhythmias in a postoperative cardiac patient, provide adequate oxygen and reduce the heart’s workload while carefully maintaining metabolic, neurologic, respiratory, and hemodynamic status.
♦ As appropriate, explain to the patient that he may undergo transcutaneous pacing as a noninvasive therapy for emergency use before he receives a temporary wire or permanent pacing wire.
♦ To avoid temporary pacemaker malfunction, install a fresh battery before each insertion. Carefully secure the external catheter wires and the pacemaker box. Assess the threshold daily. Watch closely for premature contractions, a sign of myocardial irritation.
♦ To avert permanent pacemaker malfunction, restrict the patient’s activity after insertion, as ordered. Monitor the pulse rate regularly, and watch for signs of decreased cardiac output.
♦ If the patient has a permanent pacemaker, warn him about environmental hazards, as indicated by the pacemaker’s manufacturer. Although hazards may not present a problem, 24-hour Holter monitoring may be helpful. Tell the patient to report light-headedness or syncope, and stress the importance of regular checkups.
CARDIAC TAMPONADE
Cardiac tamponade is a rapid, unchecked increase in pressure in the pericardial sac that compresses the heart, impairs diastolic filling, and reduces cardiac output. The pressure increase usually results from blood or fluid accumulation in the pericardial sac. Even a small amount of fluid (50 to 100 ml) can cause a serious tamponade if it accumulates rapidly.
Prognosis depends on the rate of fluid accumulation. If it accumulates rapidly, cardiac tamponade requires emergency lifesaving measures to prevent death. A slow accumulation and increase in pressure, as in pericardial effusion associated with malignant tumors, may not produce immediate symptoms because the fibrous wall of the pericardial sac can gradually stretch to accommodate as much as 1 to 2 L of fluid.
Causes
♦ Acute myocardial infarction
♦ Chronic renal failure requiring dialysis
♦ Connective tissue disorders (such as rheumatoid arthritis, systemic lupus erythematosus, rheumatic fever, vasculitis, and scleroderma)
♦ Drug reaction from procainamide, hydralazine, minoxidil, isoniazid, penicillin, methysergide maleate, or daunorubicin
♦ Hemorrhage from nontraumatic causes (such as anticoagulant therapy in patients with pericarditis or rupture of the heart or great vessels)
♦ Hemorrhage from trauma (such as gunshot or stab wounds to the chest or perforation by the catheter during cardiac or central venous catheterization or postcardiac surgery)
♦ Idiopathic causes (Dressler’s syndrome)
♦ Viral or postirradiation pericarditis
Pathophysiology
In cardiac tamponade, the accumulation of pericardial fluid causes increased stiffness of the ventricle, requiring higher filling pressures. The progressive accumulation of fluid in the pericardial sac causes pericardial pressure increases above the ventricular filling pressure, resulting in reduced cardiac output. This compression obstructs blood flow into the ventricles and reduces the amount of blood that can be pumped out of the heart with each contraction. (See Understanding cardiac tamponade,page 152.)
Each time the ventricles contract, more fluid accumulates in the pericardial sac. This further limits the amount of blood that can fill the ventricular chambers—especially the left ventricle—during the next cardiac cycle. A further decrease in cardiac output occurs due to equilibration of pericardial and left ventricular filling pressures.
Cardiac tamponade may cause a cardiac condition called pulseless electrical activity (PEA). In PEA, isolated electrical activity occurs sporadically without evidence of myocardial contraction. Unless the underlying cardiac tamponade is identified and treated quickly, PEA results in death.
The amount of fluid necessary to cause cardiac tamponade varies greatly; it may be as little as 50 ml when the fluid accumulates rapidly or more than 2 L when the fluid accumulates slowly and the pericardium stretches to adapt.
Signs and symptoms
♦ Elevated central venous pressure (CVP) with neck vein distention due to increased jugular venous pressure
♦ Muffled heart sounds caused by fluid in the pericardial sac
Types of cardiac arrhythmias
This chart reviews many common cardiac arrhythmias and outlines their features, causes, and treatment. Use a normal electrocardiogram strip, if available, to compare normal cardiac rhythm configurations with the rhythm strips below. Characteristics of normal sinus rhythm include:
♦ ventricular and atrial rates of 60 to 100 beats/minute
♦ regular and uniform QRS complexes and P waves
♦ PR interval of 0.12 to 0.20 second
♦ QRS duration of 0.06 to 0.10 second
♦ identical atrial and ventricular rates, with constant PR intervals.
Arrhythmia
Features
Causes Treatment
Treatment
Sinus tachycardia
♦ Atrial and ventricular rhythms regular
♦ Rate > 100 beats/minute; rarely,
> 160 beats/minute
♦ Normal P wave preceding each QRS complex
♦ Normal physiologic response to fever, exercise, anxiety, pain, dehydration; may also accompany shock, left-sided heart failure, cardiac tamponade, hyperthyroidism, anemia, hypovolemia, pulmonary embolism, and an anterior-wall myocardial infarction (MI)
♦ May also occur with atropine, epinephrine, isoproterenol, quinidine, caffeine, alcohol, cocaine, amphetamine, and nicotine use
♦ Correction of underlying cause
♦ Beta-adrenergic blocker or calcium channel blocker for symptomatic patients
Sinus bradycardia
♦ Atrial and ventricular rhythms regular
♦ Rate < 60 beats/minute
♦ Normal P waves preceding each QRS complex
♦ Normal in a well-conditioned heart, as in an athlete
♦ Increased intracranial pressure; increased vagal tone due to straining during defecation, vomiting, intubation, or mechanical ventilation; sick sinus syndrome; hypothyroidism; and an inferior-wall MI
♦ May also occur with anticholinesterase, betaadrenergic blocker, digoxin, or morphine use
♦ Correction of underlying cause
♦ For low cardiac output, dizziness, weakness, altered level of consciousness, or low blood pressure; advanced cardiac life support (ACLS) protocol for administration of atropine
♦ QRS complexes of uniform configuration and duration
♦ PR interval indiscernible
♦ No P waves, atrial activity appears as erratic, irregular, baseline fibrillatory waves
♦ Heart failure, chronic obstructive pulmonary disease, thyrotoxicosis, constrictive pericarditis, ischemic heart disease, sepsis, pulmonary embolus, rheumatic heart disease, hypertension, mitral stenosis, atrial irritation, or complication of coronary bypass or valve replacement surgery
♦ If patient’s condition is unstable with a ventricular rate > 150 beats/minute, immediate cardioversion
♦ If patient’s condition is stable, drug therapy may include a calcium channel blocker, a betaadrenergic blocker, digoxin, procainamide, quinidine, ibutilide, or amiodarone
♦ Possibly, anticoagulation therapy
♦ Possibly, dual-chamber atrial pacing, placement of an implantable atrial pacemaker, or surgical maze procedure
Junctional rhythm
♦ Atrial and ventricular rhythms regular; atrial rate 40 to 60 beats/minute; ventricular rate usually 40 to 60 beats/minute (60 to 100 beats/minute is accelerated junctional rhythm)
♦ P waves preceding, hidden within (absent), or after QRS complex; usually inverted if visible
♦ PR interval (when present) < 0.12 second
♦ QRS complex configuration and duration normal, except in aberrant conduction
♦ An inferior-wall MI or ischemia, hypoxia, vagal stimulation, and sick sinus syndrome
♦ Acute rheumatic fever
♦ Valve surgery
♦ Digoxin toxicity
♦ Correction of underlying cause
♦ Atropine for symptomatic slow rate
♦ Pacemaker insertion if patient doesn’t respond to drugs
♦ Discontinuation of digoxin if appropriate
First-degree AV block
♦ Atrial and ventricular rhythms regular
♦ PR interval > 0.20 second
♦ P wave precedes QRS complex
♦ QRS complex normal
♦ May be seen in healthy persons
♦ An inferior-wall MI or ischemia, hypothyroidism, hypokalemia, and hyperkalemia
♦ Digoxin toxicity; quinidine, procainamide, betaadrenergic blocker, calcium channel blocker, or amiodarone use
♦ Correction of underlying cause
♦ Possibly atropine if PR interval exceeds 0.26 second or symptomatic bradycardia develops
♦ Cautious use of digoxin, a calcium channel blocker, and a beta-adrenergic blocker
Second-degree AV block
Mobitz I (Wenckebach)
♦ Atrial rhythm regular
♦ Ventricular rhythm irregular
♦ Atrial rate exceeds ventricular rate
♦ PR interval progressively, but only slightly, longer with each cycle until QRS complex disappears (dropped beat); PR interval shorter after dropped beat
♦ An inferior-wall MI, cardiac surgery, acute rheumatic fever, and vagal stimulation
♦ Digoxin toxicity; propranolol, quinidine, or procainamide use
♦ Treatment of underlying cause
♦ Atropine or temporary pacemaker for symptomatic bradycardia
♦ Discontinuation of digoxin if appropriate
Second-degree AV block
Mobitz II
♦ Atrial rhythm regular
♦ Ventricular rhythm regular or irregular, with varying degree of block
♦ P-P interval constant
♦ QRS complexes periodically absent
♦ Severe coronary artery disease, an anterior-wall MI, and acute myocarditis
♦ Digoxin toxicity
♦ Atropine, dopamine, or epinephrine for symptomatic bradycardia
♦ Temporary or permanent pacemaker for symptomatic bradycardia
♦ Discontinuation of digoxin if appropriate
Third-degree AV block
Complete heart block
♦ Atrial rhythm regular
♦ Ventricular rhythm regular and rate slower than atrial rate
♦ No relation between P waves and QRS complexes
♦ No constant PR interval
♦ QRS complex normal (nodal pacemaker) or wide and bizarre (ventricular pacemaker)
♦ An inferior- or anterior-wall MI, congenital abnormality, rheumatic fever, hypoxia, postoperative complication of mitral valve replacement, postprocedure complication of radiofrequency ablation in or near AV nodal tissue, Lev’s disease (fibrosis and calcification that spreads from cardiac structures to the conductive tissue), and Lenègre’s disease (conductive tissue fibrosis)
♦ Digoxin toxicity
♦ Atropine, dopamine, or epinephrine for symptomatic bradycardia
♦ Temporary or permanent pacemaker for symptomatic bradycardia
Premature ventricular contraction (PVC)
♦ Atrial rhythm regular
♦ Ventricular rhythm irregular
♦ QRS complex premature, usually followed by a complete compensatory pause
♦ QRS complex wide and distorted, usually > 0.14 second
♦ Premature QRS complexes occurring alone, in pairs, or in threes, alternating with normal beats; focus from one (uniform) or more (multiform) sites
♦ Ominous when clustered, multifocal, with R wave on T pattern
♦ Heart failure; a previous or acute MI, ischemia, or contusion; myocardial irritation by ventricular catheter or a pacemaker; hypercapnia; hypokalemia; hypocalcemia; and hypomagnesemia
♦ Drug toxicity (digoxin, aminophylline, tricyclic antidepressant, beta-adrenergic blocker, isoproterenol, or dopamine)
♦ Caffeine, tobacco, or alcohol use
♦ Psychological stress, anxiety, pain, or exercise
♦ If warranted, procainamide, amiodarone, or lidocaine I.V.
♦ Treatment of underlying cause
♦ Discontinuation of drug causing toxicity
♦ Potassium chloride I.V. infusion if PVC induced by hypokalemia
♦ Magnesium sulfate I.V. if PVC induced by hypomagnesemia
Ventricular tachycardia
♦ Ventricular rate 140 to 220 beats/minute, rhythm usually regular
♦ QRS complexes wide, bizarre, and independent of P waves
♦ P waves not discernible
♦ May start and stop suddenly
♦ Myocardial ischemia, an MI, or aneurysm; coronary artery disease; rheumatic heart disease; mitral valve prolapse; heart failure; cardiomyopathy; ventricular catheters; hypokalemia; hypercalcemia; hypomagnesemia; and pulmonary embolism
♦ Digoxin, procainamide, epinephrine, or quinidine toxicity
♦ Anxiety
♦ With pulse: If hemodynamically stable, ACLS protocol for administration of amiodarone; if drug is ineffective, synchronized cardioversion
♦ If polymorphic VT complexes, consultation with an expert in arrhythmia management
♦ Pulseless: CPR; ACLS protocol for defibrillation, endotracheal (ET) intubation, and administration of epinephrine or vasopressin, followed by amiodarone or lidocaine and, if ineffective, magnesium sulfate
Ventricular fibrillation
♦ Ventricular rhythm and rate chaotic and rapid
♦ QRS complexes wide and irregular; no visible P waves
♦ No pulse palpable
♦ Myocardial ischemia, an MI, untreated ventricular tachycardia, R-on-T phenomenon, hypokalemia, hyperkalemia, hypercalcemia, hypoxemia, alkalosis, electric shock, and hypothermia
♦ Digoxin, epinephrine, or quinidine toxicity
♦ Pulseless: CPR; ACLS protocol for defibrillation, ET intubation, and administration of epinephrine or vasopressin, amiodarone, or lidocaine and, if ineffective, magnesium sulfate or procainamide
♦ ICD if risk for recurrent ventricular fibrillation
Asystole
♦ No atrial or ventricular rate or rhythm
♦ No discernible P waves, QRS complexes, or T waves
♦ No pulse palpable
♦ Myocardial ischemia, an MI, aortic valve disease, heart failure, hypoxia, hypokalemia, severe acidosis, electric shock, ventricular arrhythmia, AV block, pulmonary embolism, heart rupture, cardiac tamponade, hyperkalemia, and electromechanical dissociation
♦ Cocaine overdose
♦ CPR, ACLS protocol for ET intubation, transcutaneous pacing, and administration of epinephrine or vasopressin; and consider atropine.
Comparing normal and abnormal conduction
Normal cardiac conduction
The heart’s conduction system, shown below, begins at the sinoatrial (SA) node—the heart’s pacemaker. When an impulse leaves the SA node, it travels through the atria along
Bachmann’s bundle and the internodal pathways to the atrioventricular (AV) node, and then down the bundle of His, along the bundle branches and, finally, down the Purkinje fibers to the ventricles.
Abnormal cardiac conduction
Altered automaticity, reentry, or conduction disturbances may cause cardiac arrhythmias.
Altered automaticity
Altered automaticity is the result of partial depolarization, which may increase the intrinsic rate of the SA node or latent pacemakers or may induce ectopic pacemakers to reach threshold and depolarize.
Automaticity may be altered by drugs, such as epinephrine, atropine, and digoxin, and by such conditions as acidosis, alkalosis, hypoxia, a myocardial infarction (MI), hypokalemia, and hypocalcemia. Examples of arrhythmias caused by altered automaticity include atrial fibrillation and flutter; supraventricular tachycardia; premature atrial, junctional, and ventricular complexes; ventricular tachycardia and fibrillation; and accelerated idioventricular and junctional rhythms.
Reentry
Ischemia or a deformity causes an abnormal circuit to develop within conductive fibers. Although current flow is blocked in one direction within the circuit, the descending impulse can travel in the other direction. By the time the impulse completes the circuit, the previously depolarized tissue within the circuit is no longer refractory to stimulation, allowing reentry of the impulse and repetition of this cycle.
Conditions that increase the likelihood of reentry include hyperkalemia, myocardial ischemia, and the use of certain antiarrhythmics. Reentry may be responsible for such arrhythmias as paroxysmal supraventricular tachycardia; premature atrial, junctional, and ventricular complexes; and ventricular tachycardia.
An alternative reentry mechanism depends on the presence of a congenital accessory pathway linking the atria and the ventricles outside the AV junction; for example, Wolff-Parkinson-White syndrome.
Conduction disturbances
Conduction disturbances occur when impulses are conducted too quickly or too slowly. Possible causes include trauma, drug toxicity, myocardial ischemia, MI, and electrolyte abnormalities. The AV blocks occur as a result of conduction disturbances.
Understanding cardiac tamponade
The pericardial sac, which surrounds and protects the heart, is composed of several layers. The fibrous pericardium is the tough outermost membrane; the inner membrane, called the serous membrane, consists of the visceral and parietal layers. The visceral layer clings to the heart and is also known as the epicardial layer of the heart. The parietal layer lies between the visceral layer and the fibrous pericardium. The pericardial space—between the visceral and parietal layers—contains 10 to 30 ml of pericardial fluid. This fluid lubricates the layers and minimizes friction when the heart contracts.
In cardiac tamponade, blood or fluid fills the pericardial space, compressing the heart chambers, increasing intracardiac pressure, and obstructing venous return. As blood flow into the ventricles falls, so does cardiac output. Without prompt treatment, low cardiac output can be fatal.
♦ Paradoxical pulse (an inspiratory decrease in systemic blood pressure greater than 15 mm Hg) due to impaired diastolic filling
♦ Diaphoresis and cool, clammy skin caused by a decrease in cardiac output
♦ Anxiety, restlessness, and syncope due to a drop in cardiac output
♦ Cyanosis due to reduced oxygenation of the tissues
♦ Weak, rapid pulse in response to a drop in cardiac output
♦ Cough, dyspnea, orthopnea, and tachypnea due to lung compression by an expanding pericardial sac and the inability to move blood from the pulmonary vasculature into the compromised left ventricle
Complications
Reduced cardiac output (fatal without prompt treatment)
Diagnosis
♦ Chest X-rays show a slightly widened mediastinum and possible cardiomegaly. The cardiac silhouette may have a goblet-shaped appearance.
♦ Electrocardiography (ECG) may show a lowamplitude QRS complex and electrical alternans, an alternating beat-to-beat change in amplitude of the P wave, QRS complex, and T wave. Generalized ST-segment elevation is noted in all leads. An ECG is used to rule out other cardiac disorders; it may reveal changes produced by acute pericarditis.
♦ Pulmonary artery catheterization detects increased right atrial pressure, right ventricular diastolic pressure, and CVP.
♦ Echocardiography may reveal pericardial effusion with signs of right ventricular and atrial compression.
Treatment
♦ Supplemental oxygen to improve oxygenation
♦ Continuous ECG and hemodynamic monitoring in an intensive care unit to detect complications and monitor effects of therapy
♦ Pericardiocentesis (needle aspiration of the pericardial cavity) to reduce fluid in the pericardial sac and improve systemic arterial pressure and cardiac output (A catheter may be left in the pericardial space attached to a drainage container to allow for continuous fluid drainage.)
♦ Pericardial window (surgical creation of an opening) to remove accumulated fluid from the pericardial sac
♦ Pericardectomy (resection of a portion or all of the pericardium) to allow full communication with the pleura, if repeated pericardiocentesis fails to prevent recurrence
♦ Trial volume loading with crystalloids, such as I.V. normal saline solution, to maintain systolic blood pressure
♦ An inotropic drug, such as isoproterenol or dopamine, to improve myocardial contractility until fluid in the pericardial sac can be removed
♦ Blood transfusion or a thoracotomy to drain reaccumulating fluid or to repair bleeding sites may be necessary in traumatic injury
♦ The heparin antagonist protamine sulfate to stop bleeding in heparin-induced tamponade
♦ Vitamin K to stop bleeding in warfarin-induced tamponade
Special considerations
Pericardiocentesis
♦ Explain the procedure to the patient. Keep at the bedside a pericardial aspiration needle attached to a 50-ml syringe by a three-way stopcock, an ECG machine, and an emergency cart with a defibrillator. Make sure the equipment is turned on and ready for immediate use. Position the patient at a 45- to 60-degree angle. Connect the precordial ECG lead to the hub of the aspiration needle with an alligator clamp and connecting wire, and assist with fluid aspiration. When the needle touches the myocardium, you’ll see an ST-segment elevation or premature ventricular contractions.
♦ Monitor blood pressure and CVP during and after pericardiocentesis. Infuse I.V. solutions, as prescribed, to maintain blood pressure. Watch for a decrease in CVP and a concomitant increase in blood pressure, which indicate relief of cardiac compression.
♦ Watch for complications of pericardiocentesis, such as ventricular fibrillation, vasovagal response, or coronary artery or cardiac chamber puncture. Closely monitor ECG changes, blood pressure, pulse rate, level of consciousness, and urine output.
Thoracotomy
♦ Explain the procedure to the patient. Tell him what to expect postoperatively (chest tubes, drainage bottles, and administration of oxygen). Teach him how to turn, deep breathe, and cough.
♦ Give an antibiotic, protamine sulfate, or vitamin K, as ordered.
♦ Postoperatively, monitor critical parameters, such as vital signs and arterial blood gas values, and assess heart and respiratory rates. Give pain medication, as ordered. Maintain the chest drainage system, and be alert for complications, such as hemorrhage and arrhythmias.
CARDIOMYOPATHY
Cardiomyopathy generally applies to disease of the heart muscle fibers, and it occurs in three main forms: dilated, hypertrophic, and restrictive (extremely rare). Cardiomyopathy is the second most common direct cause of sudden death; coronary artery disease (CAD) is the first. About 5 to 8 per 100,000 Americans have dilated cardiomyopathy, the most common type. At greatest risk for dilated cardiomyopathy are males and blacks; other risk factors include CAD, hypertension, pregnancy, viral infections, and alcohol or illegal drug use. Because dilated cardiomyopathy usually isn’t diagnosed until its advanced stages, the prognosis is generally poor.
There are two types of hypertrophic cardiomyopathy. The more common form—nonobstructive hypertrophic cardiomyopathy—is caused by pressure overload-hypertension or aortic valve stenosis. Hypertrophic obstructive cardiomyopathy (HOCM) is due to a genetic abnormality. The course of hypertrophic cardiomyopathy varies. Some patients progressively deteriorate, whereas others remain stable for years. It’s estimated that almost 50% of all sudden deaths in competitive athletes age 35 or younger are due to HOCM. If severe, restrictive cardiomyopathy is irreversible.
Causes
Most patients with dilated cardiomyopathy have idiopathic, or primary, disease but some are secondary to identifiable causes. (See Comparing cardiomyopathies,pages 156 and 157.) HOCM is almost always inherited as a non-sex-linked autosomal dominant trait.
Pathophysiology
Dilated cardiomyopathy results from extensively damaged myocardial muscle fibers. Consequently, there’s reduced contractility in the left ventricle. As systolic function declines, stroke volume, ejection fraction, and cardiac output fall. As end-diastolic volumes rise, pulmonary congestion may occur. The elevated end-diastolic volume is a compensatory response to preserve stroke volume, despite a reduced ejection fraction. The sympathetic nervous system is also stimulated to increase heart rate and contractility. The kidneys are stimulated to retain sodium and water to maintain cardiac output, and vasoconstriction also occurs as the renin-angiotensin-aldosterone system is stimulated. When these compensatory mechanisms can no longer maintain cardiac output, the heart begins to fail. Left ventricular dilation occurs as venous return and systemic vascular resistance rise. Eventually, the atria also dilate as more work is required to pump blood into the full ventricles. Cardiomegaly occurs as a consequence of dilation of the atria and ventricles. Blood pooling in the ventricles increases the risk of emboli.
Barth syndrome is a rare genetic disorder that can cause dilated cardiomyopathy in boys. This syndrome may be associated with skeletal muscle changes, short stature, neutropenia, and increased susceptibility to bacterial infections. Evidence of dilated cardiomyopathy may appear as early as the first few days or months of life.
Only gold members can continue reading. Log In or Register to continue
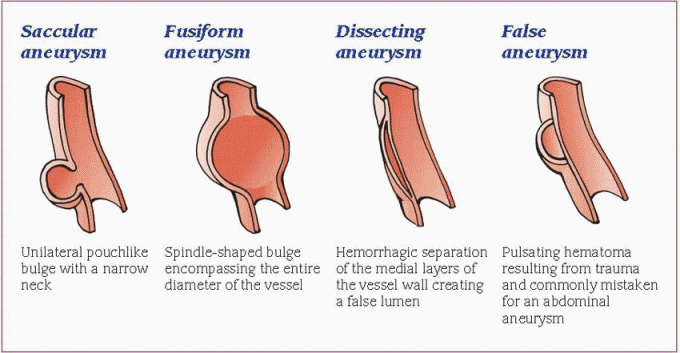
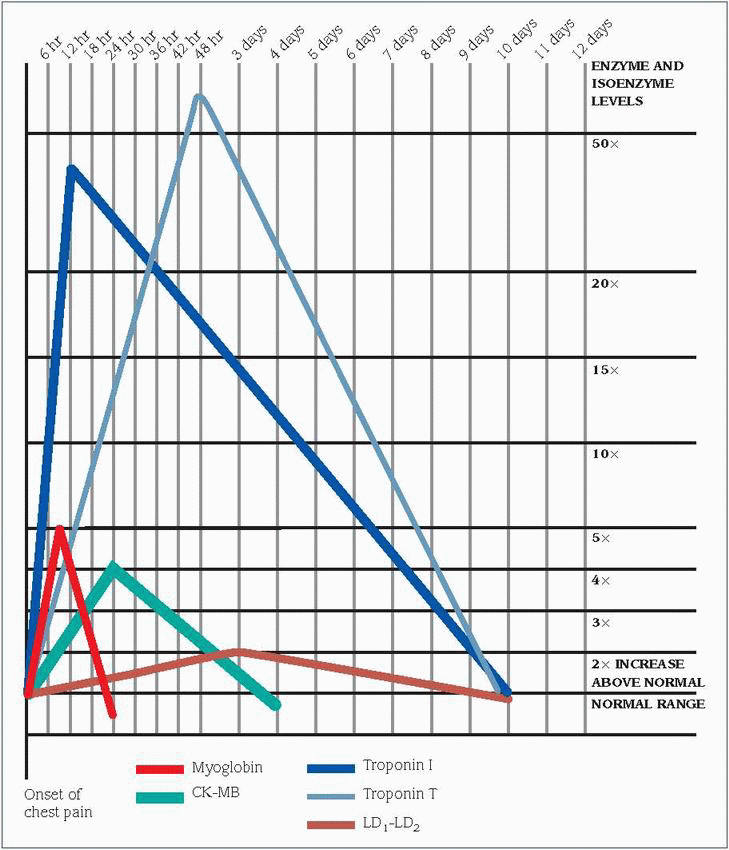
 Be alert for signs of rupture, which may be immediately fatal. Watch closely for signs of acute blood loss, such as decreasing blood pressure; increasing pulse and respiratory rate; cool, clammy skin; restlessness; and decreased sensorium.
Be alert for signs of rupture, which may be immediately fatal. Watch closely for signs of acute blood loss, such as decreasing blood pressure; increasing pulse and respiratory rate; cool, clammy skin; restlessness; and decreased sensorium.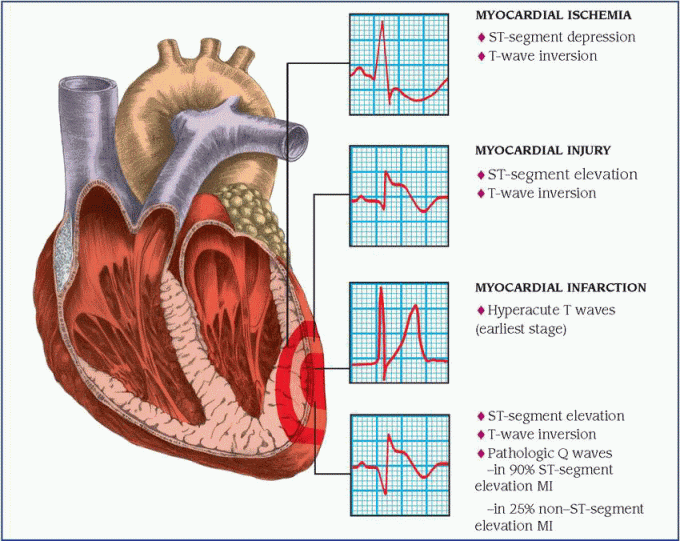
 Females may experience typical chest pain with acute ischemia and an MI; however, females—and occasionally males, elderly patients, and those patients with diabetes—may also experience atypical chest pain. Signs and symptoms include upper back discomfort between the shoulder blades, palpitations, a feeling of fullness in the neck, nausea, abdominal discomfort, dizziness, unexplained fatigue, and exhaustion or shortness of breath.
Females may experience typical chest pain with acute ischemia and an MI; however, females—and occasionally males, elderly patients, and those patients with diabetes—may also experience atypical chest pain. Signs and symptoms include upper back discomfort between the shoulder blades, palpitations, a feeling of fullness in the neck, nausea, abdominal discomfort, dizziness, unexplained fatigue, and exhaustion or shortness of breath.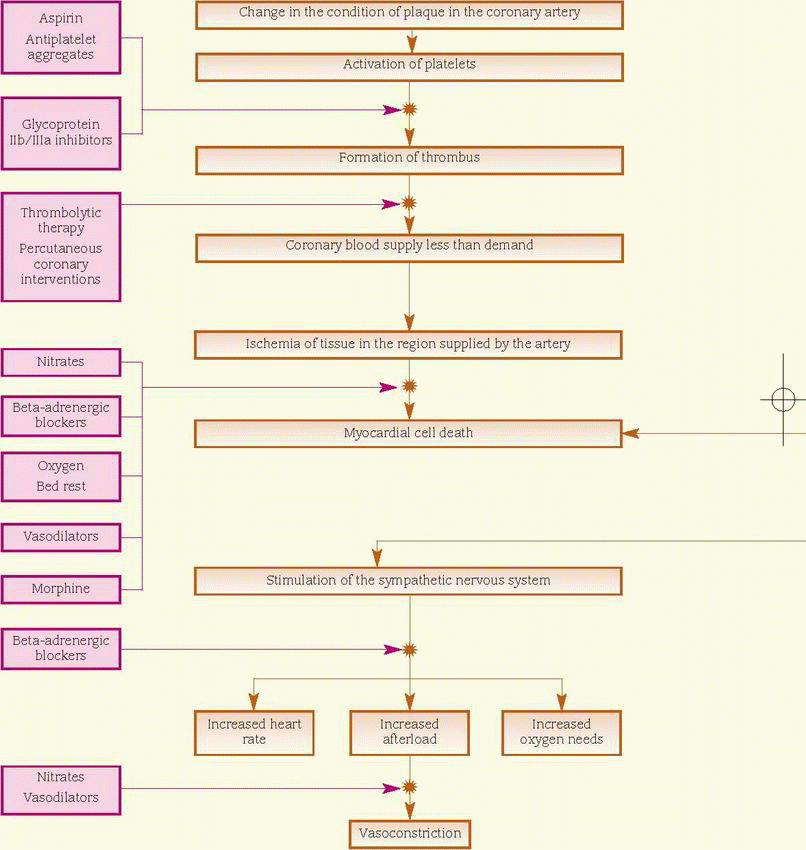
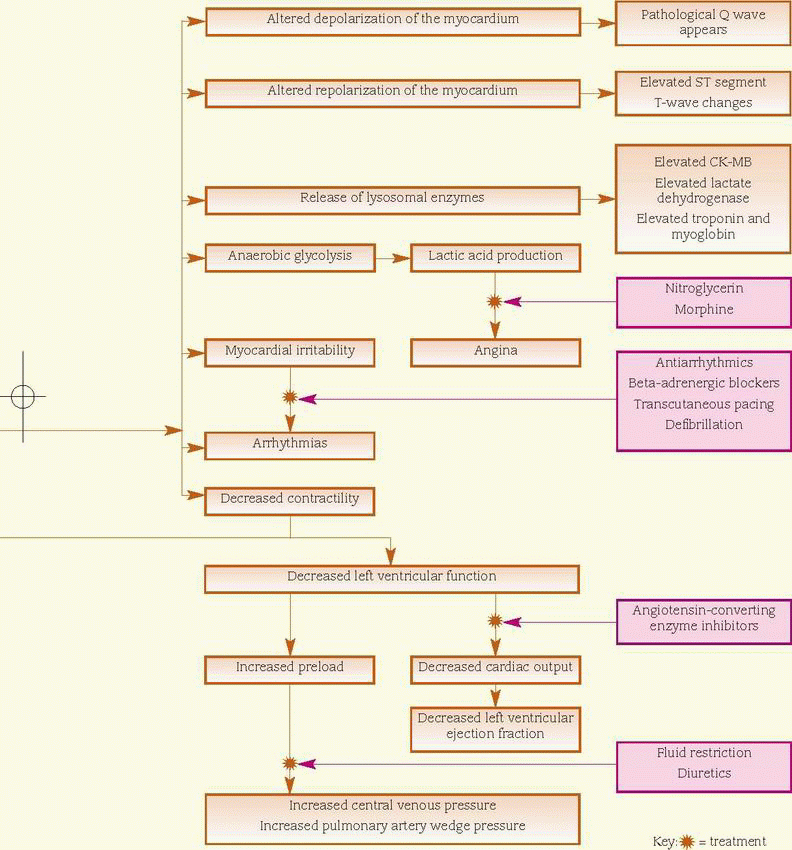
 Aging causes sclerotic changes in blood vessels, which leads to decreased elasticity and narrowing of the lumen, further contributing to the development of arterial occlusive disease. In people older than age 70, the prevalence of the disease is estimated to be 10% to 18%.
Aging causes sclerotic changes in blood vessels, which leads to decreased elasticity and narrowing of the lumen, further contributing to the development of arterial occlusive disease. In people older than age 70, the prevalence of the disease is estimated to be 10% to 18%. An infant may be cyanotic because he has a cardiac or pulmonary disorder. Cyanosis that worsens with crying is most likely associated with cardiac causes because crying increases pulmonary resistance to blood flow, resulting in an increased right-to-left shunt. Cyanosis that improves with crying is most likely associated with pulmonary causes because deep breathing improves tidal volume.
An infant may be cyanotic because he has a cardiac or pulmonary disorder. Cyanosis that worsens with crying is most likely associated with cardiac causes because crying increases pulmonary resistance to blood flow, resulting in an increased right-to-left shunt. Cyanosis that improves with crying is most likely associated with pulmonary causes because deep breathing improves tidal volume. Cardiac tamponade may cause a cardiac condition called pulseless electrical activity (PEA). In PEA, isolated electrical activity occurs sporadically without evidence of myocardial contraction. Unless the underlying cardiac tamponade is identified and treated quickly, PEA results in death.
Cardiac tamponade may cause a cardiac condition called pulseless electrical activity (PEA). In PEA, isolated electrical activity occurs sporadically without evidence of myocardial contraction. Unless the underlying cardiac tamponade is identified and treated quickly, PEA results in death.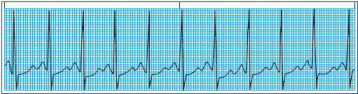
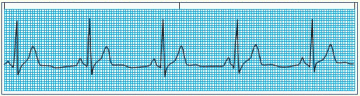
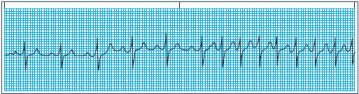
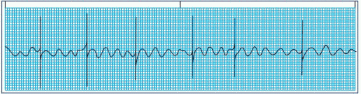
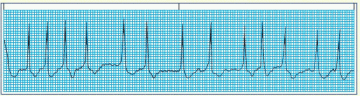
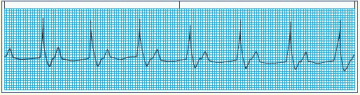
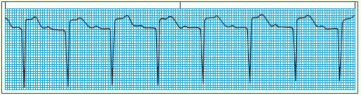
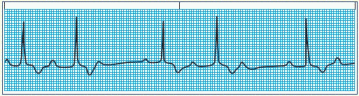
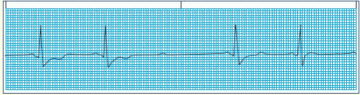
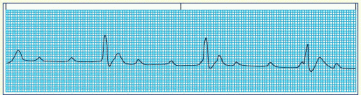
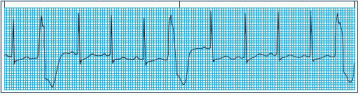
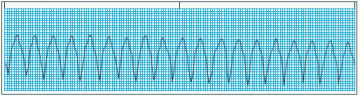
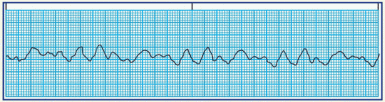
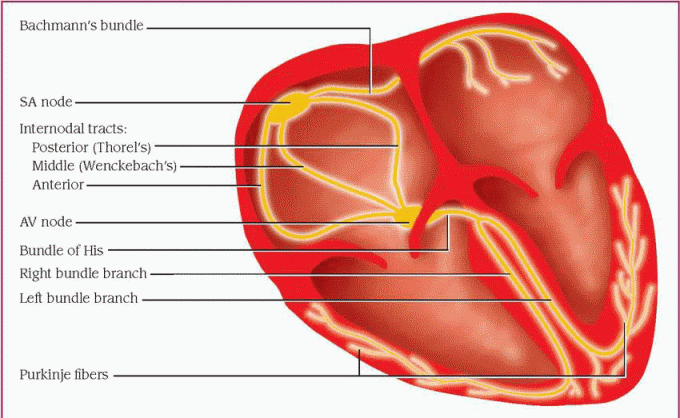
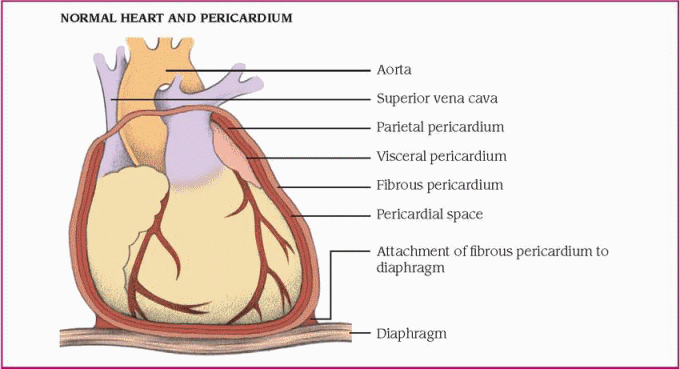
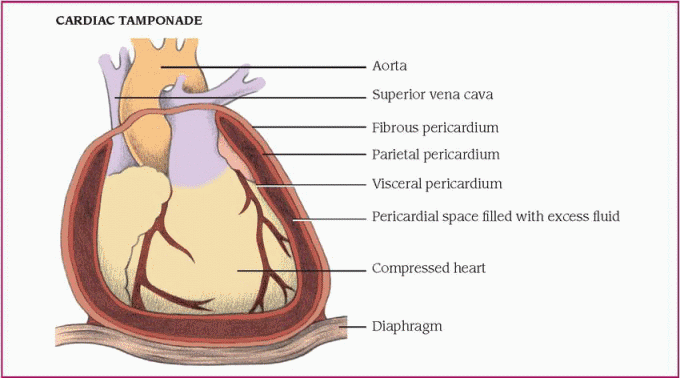
 Barth syndrome is a rare genetic disorder that can cause dilated cardiomyopathy in boys. This syndrome may be associated with skeletal muscle changes, short stature, neutropenia, and increased susceptibility to bacterial infections. Evidence of dilated cardiomyopathy may appear as early as the first few days or months of life.
Barth syndrome is a rare genetic disorder that can cause dilated cardiomyopathy in boys. This syndrome may be associated with skeletal muscle changes, short stature, neutropenia, and increased susceptibility to bacterial infections. Evidence of dilated cardiomyopathy may appear as early as the first few days or months of life.


