CT of 2nd Branchial Cleft Cyst Axial contrast-enhanced CT reveals a 2nd branchial cleft cyst (BCC) located posterior to the submandibular gland , lateral to the carotid space , and anterior to the sternomastoid muscle . Capsule thickening suggests inflammation.
Gross Photo of Branchial Cleft Cyst The resection specimen includes a benign lymph node , separate from the cyst immediately below. Note the thick, fibrous connective tissue wall surrounding the cyst, filled with hemorrhagic and keratinaceous material.
Keratinaceous Debris in Branchial Cleft Cyst The lumen of this BCC is filled with keratinaceous debris. There is a thin, squamous epithelium without any atypia. There is a germinal center within the associated lymphoid tissue.
Metaplastic Squamous-Lined Cyst The cyst is lined by metaplastic squamous epithelium subtended by a very thin basement membrane between the epithelium and lymphoid tissue. Metaplasia is usually seen in patients who have had previous infection.
TERMINOLOGY
Abbreviations
• Branchial cleft cyst (BCC)
Synonyms
• Lateral neck cyst
• Cervical lymphoepithelial cyst
Definitions
• By convention, BCC refers to congenital developmental lateral cervical cyst derived from remnants of 2nd branchial apparatus
~ 80-90% of all branchial anomalies arise from 2nd branchial apparatus
• Embryogenesis usually complete by 6-7 weeks of gestation
• Failure of obliteration of cervical sinus results in 2nd branchial cleft remnant (cyst, sinus, or fistula)
Sinus is respiratory epithelium lined, but squamous metaplasia and lymphoid hyperplasia develop as consequence of immunologic stimulation during infection
• 2nd branchial cleft fistula extends from skin anterior to sternocleidomastoid muscle (SCM), through carotid artery bifurcation to terminate in tonsillar fossa
• 3rd and 4th BCCs are very uncommon (< 5%)
Recurrent neck abscess or acute suppurative thyroiditis
Vast majority on left side (90-95%)
• Some authors posit cystic transformation of cervical lymph nodes (specifically in adults)
CLINICAL ISSUES
Epidemiology
• Incidence
Uncommon
– Still, BCC are 1 of most commonly encountered congenital anomalies in pediatric otolaryngic practice
– Thyroglossal duct cysts are most common
BCC accounts for ~ 20% of all congenital cervical cysts
– Cysts > > sinuses (3:1)
~ 80-90% of all branchial cleft anomalies are 2nd BCCs
4th branchial cleft anomalies are rare and involve larynx (neonatal stridor and recurrent deep neck infection)
• Age
Bimodal presentation
– < 5 years old (24%)
– 20-40 years old (75%)
– ~ 1% in > 50 years
• Sex
Equal gender distribution
Site
• Lateral neck near mandibular angle
• Along anterior border of SCM
Anywhere from hyoid bone to suprasternal notch
• Curiously, left-sided predominance for 4th branchial anomalies (> 90%)
Presentation
• Painless cervical swelling
Along anterior border of SCM
Often present for long duration
May be painful (if infected)
• Waxing and waning lesion
Frequently enlarges in concert with upper respiratory tract infection
Patients present during phase of recent enlargement
May lie dormant (clinically silent) for years
• Compressible, fluctuant
• Mucoid or pus-like secretions from sinus tract skin opening (when opening is present)
Patients present with external fistulae ± internal opening
• Clinically, some lesions may mimic parotid mass or odontogenic infection
• Bilateral lesions are usually identified in syndromic or familial association
• Clinically, 1st or 4th BCC more likely to have incision and drainage procedures, resulting in recurrence
• Important: Must consider metastatic cystic squamous cell carcinoma (SCC) in adults
Endoscopic Findings
• Advocated as part of initial assessment of neck cyst
Assess internal opening or draining sinus/fistula
Natural History
• Repeated infections and inflammation
Treatment
• Options, risks, complications
Initial work-up of suspected branchial cleft anomaly (in order)
– Intravenous or oral antibiotics (if infected)
– Fine-needle aspiration
– Endoscopy (concurrent with surgery in some cases)
– Radiographic studies
– Surgery in nonresolving cases
Avoid repeated incision and drainage, as it yields high recurrence rate
Noninfected lesions are more easily removed than infected lesions
Entire fistula tract must be removed to prevent recurrence
Complications include possible wound infection and cranial nerve paresis
• Surgical approaches
Combined simultaneous endoscopic identification of sinus tract with lateral external cervical dissection
– Cauterization of fistula used by some practitioners
Only gold members can continue reading. Log In or Register to continue



 located posterior to the submandibular gland
located posterior to the submandibular gland  , lateral to the carotid space
, lateral to the carotid space  , and anterior to the sternomastoid muscle
, and anterior to the sternomastoid muscle  . Capsule thickening suggests inflammation.
. Capsule thickening suggests inflammation.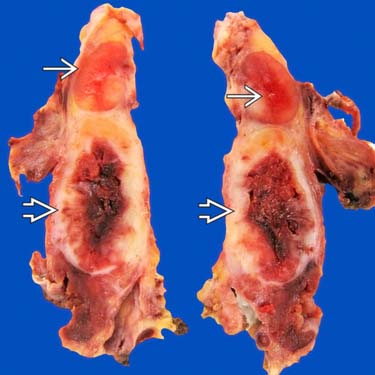
 , separate from the cyst immediately below. Note the thick, fibrous connective tissue wall
, separate from the cyst immediately below. Note the thick, fibrous connective tissue wall  surrounding the cyst, filled with hemorrhagic and keratinaceous material.
surrounding the cyst, filled with hemorrhagic and keratinaceous material.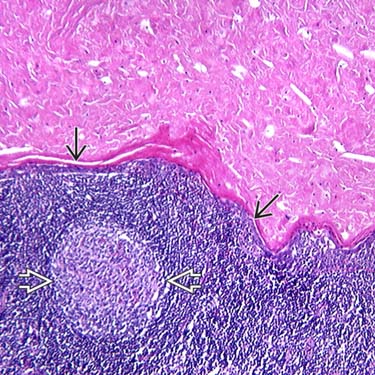
 without any atypia. There is a germinal center
without any atypia. There is a germinal center  within the associated lymphoid tissue.
within the associated lymphoid tissue.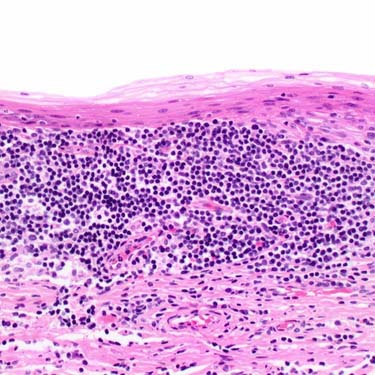

























 Combined simultaneous endoscopic identification of sinus tract with lateral external cervical dissection
Combined simultaneous endoscopic identification of sinus tract with lateral external cervical dissection



