• Elevated serum IgG4 (not invariably present, and not diagnostic of autoimmune pancreatitis)
More common in type 1 than type 2 AIP
• Steroid therapy is usually very effective
Recurrence reported in 6-26%
• Often mimics pancreatic adenocarcinoma clinically and radiographically
Macroscopic
• Enlarged, firm pancreas ± mass lesion; may mimic adenocarcinoma
Usually head is most prominently involved
• Stenosis of pancreatic duct and intrapancreatic common bile duct are common
Microscopic
• Dense, lymphoplasmacytic infiltration centered around main and interlobular pancreatic ducts
• Periductal, lobular, and perilobular fibrosis
• Obliterative phlebitis and venulitis
• 2 main types
Type 1: Lobular and interlobular distribution, obliterative phlebitis, numerous IgG4(+) plasma cells
Type 2: Duct-centric distribution, granulocytic epithelial lesions, only rare IgG(+) plasma cells
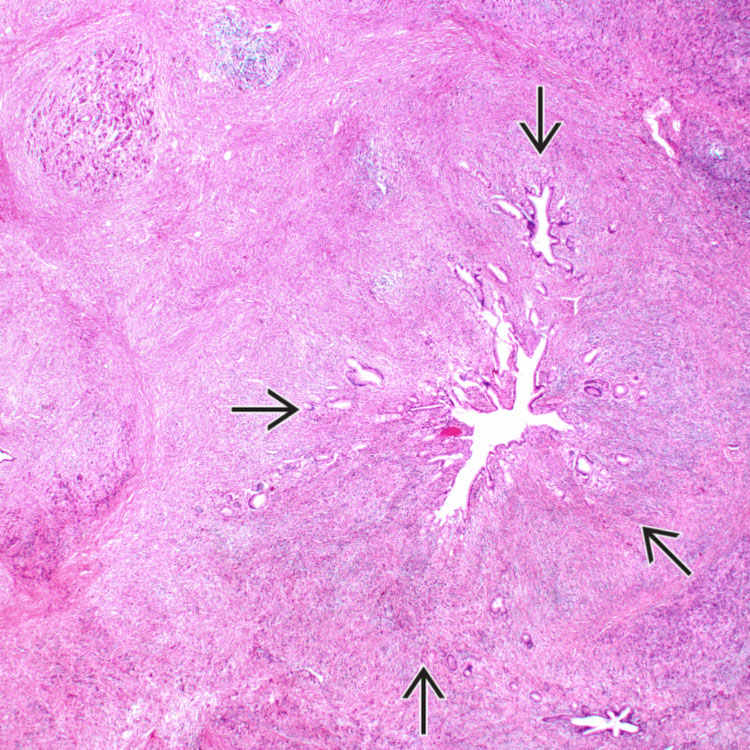
Surgical Specimen This pancreatic resection from a case of type 1 autoimmune pancreatitis (AIP) shows a dense, infiltrative, fibrotic process in the head of the pancreas.
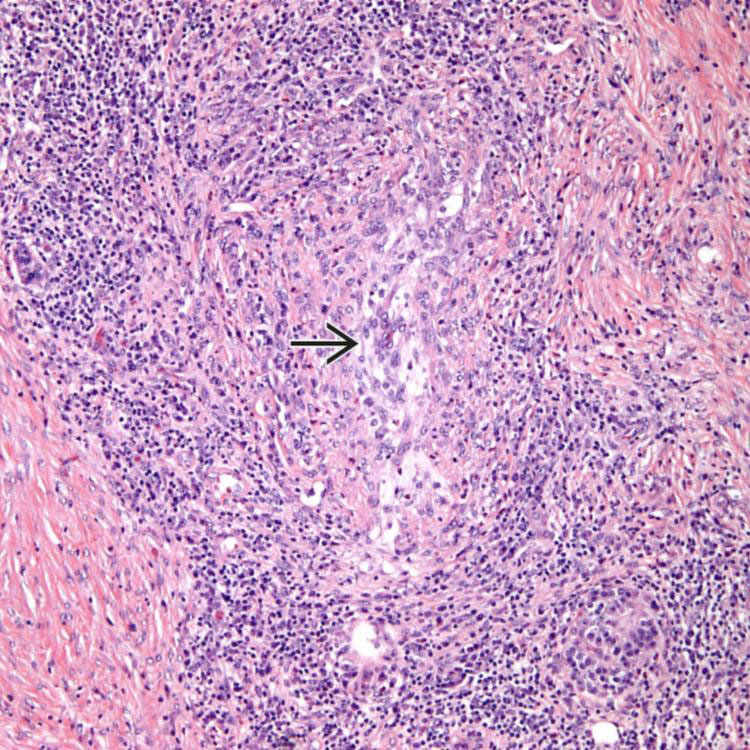
Periductal Inflammation, Type 1 Autoimmune Pancreatitis Low-power view of type 1 AIP shows marked chronic inflammation surrounding a large duct and involving the periductal stroma .
Phlebitis, Type 1 Autoimmune Pancreatitis This vein has been infiltrated by inflammatory cells, with resultant edema and destruction of the wall of the vessel. Note the surrounding fibrosis.
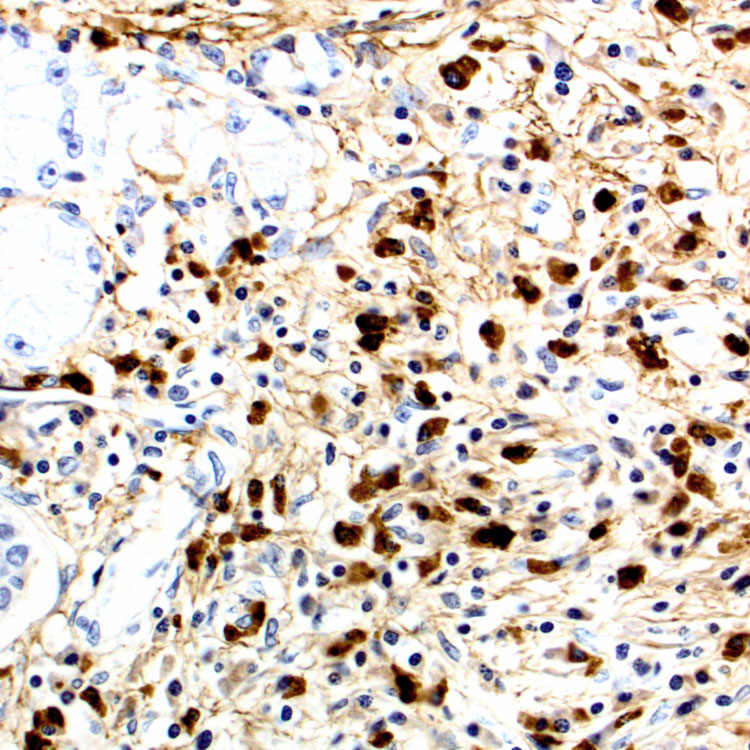
IgG4 Immunostain, Type 1 IgG4 stain in type 1 AIP shows a large number of IgG4(+) plasma cells (> 10/HPF) in the periductal stroma.
 Similar fibroinflammatory process often affects other organs such as bile ducts, salivary glands, retroperitoneum, and lymph nodes
Similar fibroinflammatory process often affects other organs such as bile ducts, salivary glands, retroperitoneum, and lymph nodes





 .
.
 has been infiltrated by inflammatory cells, with resultant edema and destruction of the wall of the vessel. Note the surrounding fibrosis.
has been infiltrated by inflammatory cells, with resultant edema and destruction of the wall of the vessel. Note the surrounding fibrosis.