Chapter 16 After studying this chapter, the learner will be able to: • Identify the components of appropriate OR attire worn in specific areas of the surgical suite. • Identify the components of personal protective equipment (PPE) donned before performing surgical hand cleansing. • Identify the sterile parameters of a surgical gown. • Demonstrate the correct method of gowning and gloving before establishing the sterile field. • Demonstrate the appropriate method of changing a contaminated glove during a surgical procedure. • Demonstrate the proper method for removing a contaminated gown and gloves. Antiseptic soap or cleanser used for cleaning the skin of patients and caregivers that has a fast-acting, broad-spectrum action to reduce the count of microorganisms before a surgical procedure. Appropriate OR attire consists of body covers such as a two-piece pantsuit, head cover, mask, and shoe covers (shoe covers are used as appropriate). Physical or mechanical obstacle between a person and a hazardous substance or microorganism. Applying or donning gloves using one of the following methods: A method of self-applying gloves while the hands are concealed within the cuffs of a sterile gown. The wearer applies two pair of sterile gloves. The inner gloves should be one half size larger than the outer glove to create a comfortable air cushion. The inner glove can be a different color to help detect a tear in the outer glove. Wearing two gloves of the same size can cause compression of the median nerve and aggravate carpal tunnel syndrome in some susceptible people. A method of self-applying gloves while the hands are exposed with or without a sterile gown. This is how gloves are reapplied after a contaminated glove is removed by the circulating nurse. The cuffs are not pulled back over the hands because they are absorbent and considered contaminated. A method for applying sterile gloves to another person who has his or her hands exposed through the cuffs of a sterile gown Applying a sterile gown to self or other member of the sterile team. Condition of the hands or decontamination with a brush and antiseptic agent or antiseptic gel. Specialized gloves worn on the inside that reveal color, commonly green or blue, when the outer glove is punctured. Personal protective equipment (PPE) Eyewear, mask, hair cover, shoe covers, gown, apron, and/or gloves worn to prevent airborne, droplet, or contact-based transmission of potentially hazardous substances or microorganisms between caregiver and patient. Attire intended for wear in the OR. Consists of basic appropriate attire for the OR with the addition of sterile gown and sterile gloves. Under the fingernails. Surgical hand hygiene (surgical scrub) Process by which the hands and arms of the team are rendered clean by mechanical and chemical action before a surgical procedure. OR attire consists of body covers such as a two-piece pantsuit, head cover, mask, and shoe covers, as appropriate. Each has an appropriate purpose to combat sources of contamination exogenous (external) to the patient. A sterile gown and gloves are added to this basic attire for sterile team members at the sterile field. Appropriate attire is a part of aseptic environmental control that also protects personnel against exposure to communicable diseases and hazardous materials. Personal protective equipment (PPE) such as eyewear and other protective items are worn by personnel as appropriate for anticipated exposure to blood and body fluids. Box 16-1 describes attire for the OR according to specific areas. 1. Dressing rooms located in the unrestricted area adjacent to the semirestricted area of the OR suite are reached through the outer unrestricted corridor. Street clothes are not worn beyond the unrestricted area. 2. Only approved, freshly laundered attire intended for use in the OR is worn within the semirestricted and restricted areas. This policy applies to everyone entering the OR suite, both professional and nonprofessional personnel and visitors. Home laundering of scrub suits may cause cross-contamination between hospital and home microflorae. Laundry conditions at home are not controlled for temperature and cleaning products and may not consistently take microbial counts to an irreducible minimum.2 a. Clean, fresh attire is donned each time on arrival in the OR suite and as necessary at other times if the attire becomes wet or grossly soiled. Blood-stained or soiled attire, including shoe covers, is not only unattractive but can also be a source of cross-contamination. Soiled attire is not worn outside the OR suite. b. An adequate supply of clean scrub suits should always be available and laundered daily, preferably in the hospital’s laundry facilities. It should not be taken home for laundering because standardized sanitation processes may not be followed. The risk for contamination of family members might be increased if clothing were contaminated with resistant microorganisms (e.g., prions causing Creutzfeldt-Jakob disease, or Mycobacterium tuberculosis causing tuberculosis [TB]). c. Masks should be changed between patients and whenever wet or soiled. 3. OR attire should not be worn outside the OR suite or outdoors. This protects the OR environment from microorganisms inherent in the outside environment and protects the outside from contamination normally associated with the OR. Before leaving the OR suite, everyone should change to street clothes. Surgeons who wear scrubs back and forth to the office place their patients at risk for exposure, and their appearance is unprofessional. a. On occasion, such as for lunch breaks, a single-use cover gown or other jacket may be worn over OR attire outside the suite. The practice of wearing cover gowns is not encouraged. After a gown is worn, it should be placed in a laundry hamper or if it is disposable it should be discarded. Some hospitals provide lab coats. These are completely buttoned and worn only once. b. OR attire should not be hung or put in a locker for wearing a second time. It should be discarded in the trash or put in a laundry hamper after one use, as appropriate. Shoes should be stored on the bottom shelf or under the locker. 4. Impeccable personal hygiene is emphasized. Each person should bathe daily with an antimicrobial and apply deodorant as appropriate. Body odor is the result of microorganisms in the hair-bearing areas of the body. This becomes unpleasant when confined to an OR while wearing a gown and gloves under hot lights. This is augmented when working with pediatric or geriatric patients where the room temperature has been intentionally elevated for patient care. a. A person with an acute infection, such as a cold or sore throat, should not be permitted within the OR suite. Personnel with cuts, burns, or skin lesions should not scrub or handle sterile supplies because serum, a bacterial medium, may seep from the eroded area. An open skin lesion may be a portal of entry for cutaneous contact with bloodborne pathogens. b. Some sterile team members who are known carriers of pathogenic microorganisms should be treated with appropriate antibiotics until nasopharyngeal culture findings are negative. c. Fingernails should be kept short (i.e., should not extend past the fingertips). Routine manicures prevent cracked cuticles and hangnails. Subungual areas harbor the majority of microorganisms on hands. Fresh nail polish on short, healthy nails may not alter the microbial count on fingernails. Polish may seal crevices. However, damaged nails and chipped or peeling polish may provide a harbor for microorganisms. Studies have shown that artificial nails and other enhancers harbor organisms, especially fungi and gram-negative bacilli. These are prohibited from the OR. d. Jewelry, including rings and watches, should be removed before entering semirestricted and restricted areas. Organisms may be harbored under rings, thus preventing effective handwashing. Necklaces or chains can grate on the skin, increasing desquamation. They might break and fall into a wound or contaminate a sterile field. Pierced-ear studs should be confined within the head cover. Dangling earrings are inappropriate in the OR. e. Facial makeup should be minimal. f. Eyewear or spectacles should be wiped with a cleaning solution before each surgical procedure and secured to the face with a head strap to prevent slippage. g. External apparel that does not serve a functional purpose should not be worn. Identification badges should be secured to prevent their contact with the sterile field or equipment used for patient care. h. Hands are washed frequently and thoroughly to remove bioburden. Washing before and after using the restroom can reduce the risk of self-contamination. Using hand cream regularly helps prevent chapped, dry skin. Bacteriostatic varieties may help reduce microbial counts on the skin. Hand sanitizer can be of benefit in reducing flora. 5. Comfortable, supportive shoes should be worn to minimize fatigue and for personal safety. Shoes should have enclosed toes and heels. Clogs may not provide a safe surface for fast walking or running during an emergency, especially while pushing a crash cart. Cloth shoes do not offer protection against spilled fluids or sharp items that may be dropped or kicked. Shoes are cleaned frequently, whether or not shoe covers are worn. Each item of OR attire is a specific means for containment of or protection against the potential sources of environmental contamination, including skin, hair, and nasopharyngeal flora and microorganisms in air, blood, and body substances. Scrub suits and head covers are worn by all personnel in the semirestricted areas of the OR suite (Fig. 16-1). Masks also are worn in the restricted areas. Additional items, such as protective eyewear, gloves, and shoe covers, are worn during a surgical procedure and for protection during hazardous exposure. • They are at least 95% efficient in filtering microbes from droplet particles in exhalations and also filter inhalations. A fluid-resistant mask is advantageous. • They are cool, comfortable, and nonobstructive to respiration. • They are nonirritating to the skin. Disposable masks are made of polypropylene, polyester, or rayon fibers. Some have fiberglass filters. Sensitive persons should try another brand. • Mask styles include rectangle shapes with four strings or cup-shaped, formed masks with an elastic band that fits around the head. • High-efficiency particulate air (HEPA) filtration masks are cup shaped and are worn when working with patients who have TB. Employers should have each employee fitted so the size worn will be known. The patient should wear a mask during transport as well. • Laser masks are high-filtration masks worn when plume from a laser or electrosurgical unit is in the environment. These masks filter airborne viruses. Masks are designed with pleats or are conical, like a cup, for a close fit, but improper application can negate their efficiency. The strings should be tied tightly, if this is the method of securing the mask, to prevent the strings from coming loose during the surgical procedure. The upper strings are tied at the back of the head; the lower strings are tied behind the neck (Fig. 16-2). The strings are never crossed over the head, because this distorts the contours of the mask along the cheeks. 1. Handle the mask only by the strings, thereby keeping the facial area of a fresh mask clean and the hands uncontaminated by a soiled mask. Do not handle the mask excessively. 2. Never lower the mask to hang loosely around the neck, never place the mask on top of the head, and never place the mask in a pocket. Avoid disseminating microorganisms. 3. Promptly discard the mask into the proper receptacle on removal. Remask with a fresh mask between patients. 4. Change the mask frequently. Do not permit the mask to become wet. Limit talking to a minimum. a. A decontamination apron worn over the scrub suit protects against liquids and cleaning agents during cleaning procedures. It should be a full-front barrier. These are usually disposable plastic. b. Fluidproof aprons are worn by sterile team members under permeable reusable sterile gowns when extensive blood loss or irrigation is anticipated. They should be lightweight and full front. These are usually disposable plastic. c. Lead aprons worn under sterile gowns protect against radiation exposure during procedures performed under fluoroscopy or image intensification or when personnel are exposed to radioactive implants. Lead aprons may be full front, full circumferential body cover, or vest and skirt style. a. Eyewear or a face shield is worn whenever a risk exists of blood or body substances from the patient splashing into the eyes of sterile team members. Bone chips and splatter can be projected from bone-cutting instruments. Several styles of goggles and eyeglasses with top and side shields fit securely against the face. Antifog goggles fit over prescription eyeglasses. A combination surgical mask with a visor eye shield or a chin-length face shield is another option. Care is taken that the lower edge of the face shield does not touch the front of the gown. Side shields applied to spectacles may not be adequate protection for random splashes. b. Laser eyewear is worn for eye protection from laser beams. Lenses of the proper optical density for each type of laser should be available and worn. An extra pair should be placed on the outer door for personnel who may need to enter the room during the procedure. The color of the glasses has no bearing on which laser light is blocked. Many manufacturers have tried to create clear lenses to minimize visual distortion c. Protective eyewear, preferably a face shield, should be worn by personnel handling or washing instruments when this activity could result in a splash, spray, or splatter to the eyes or face. Eyewear should be worn when cleaning the room to avoid splashing chemical germicides into eyes during mopping or cleaning. Surgical hand and arm scrubbing and patient skin prepping can release aerosolized antiseptic solution into the air. Protective eyewear should always be worn when working with detergent-based prep solution. d. Eyewear or a face shield that becomes contaminated should be decontaminated or discarded promptly. a. Nonsterile latex or vinyl gloves are worn to handle any material or items contaminated by blood and body substances. Gloves should be worn only during the period of contact, not continuously. Gloves are never washed between patient contacts; they are discarded. Clean objects and sterile packages should not be handled with contaminated gloves. Avoid opening cupboard doors, using a keyboard, or adjusting monitor settings while wearing soiled gloves. b. Sterile gloves are worn by sterile team members and for all invasive procedures. Sterile Kevlar-woven glove liners may be worn over or under gloves to protect the hands from cuts caused by heavy instrumentation. Liners can be worn between two layers of gloves and should be one half size larger to prevent constriction. If double-gloving, the first pair of gloves can be colored to serve as an indicator glove. If the outer glove is punctured the color shows through to make the perforation visible. c. Lead and radiation protective gloves may be needed for protection from scatter during ionizing radiation exposure for diagnostic and therapeutic procedures that use real-time imaging. The surgeon may wear natural rubber gloves impregnated with lead for procedures performed under fluoroscopy. The lead is not in direct contact with skin. Lead gloves are available in powdered and nonpowdered styles. When evaluating radiation protective gloves, be sure to note whether they are protective when used in direct radiation beams or if they are intended for use as protection from scatter. Not all radiation protective gloves are intended for use in direct beams. Radiation protective gloves without lead are commercially available.
Appropriate attire, surgical hand hygiene, and gowning and gloving
Appropriate operating room attire
Purpose of appropriate attire
Definition
Considerations for appropriate attire
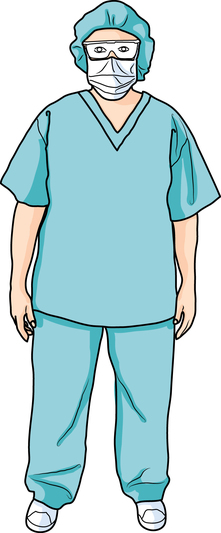
Components of appropriate attire
Mask
Personal protective equipment (PPE)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



 Website
Website