Amyloid deposits are congophilic and show “apple green” birefringence under polarized light






Top Differential Diagnoses
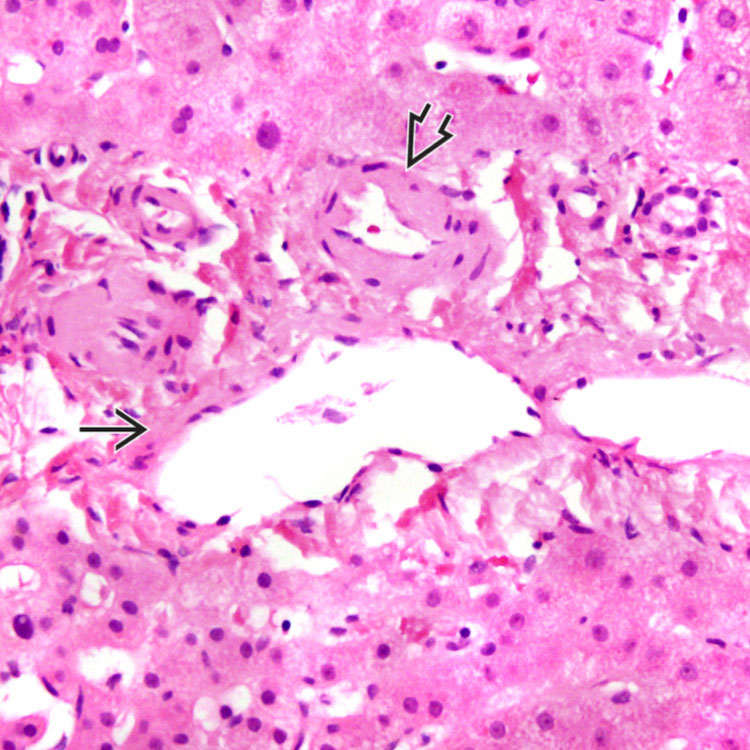
Deposits are seen in the hepatic arteriole
 and portal vein
and portal vein  in the vascular pattern of hepatic amyloidosis. This distribution is characteristic, but not specific, for the AA form.
in the vascular pattern of hepatic amyloidosis. This distribution is characteristic, but not specific, for the AA form.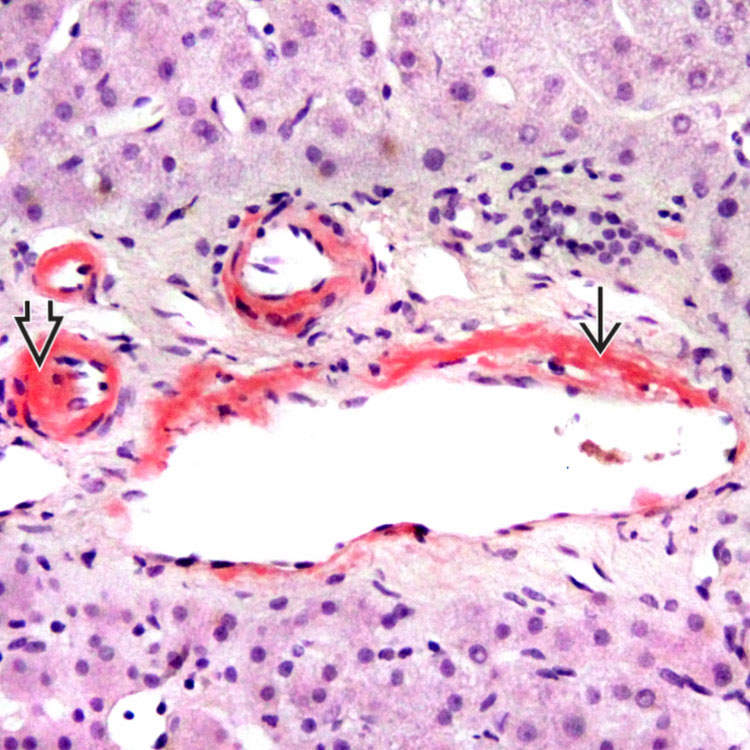
Congo red stain highlights the vascular distribution of amyloid deposits in the hepatic arteriole
 and portal vein
and portal vein  .
.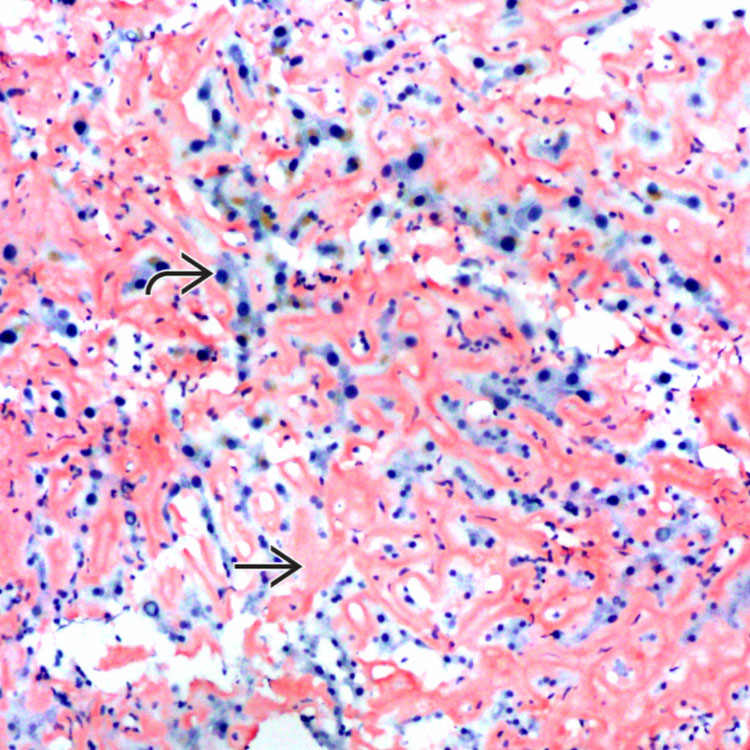
Congo red stain highlights the diffuse sinusoidal pattern
 of hepatic amyloidosis. The amyloid deposits are compressing the hepatocytes
of hepatic amyloidosis. The amyloid deposits are compressing the hepatocytes  , leading to hepatic plate atrophy.
, leading to hepatic plate atrophy.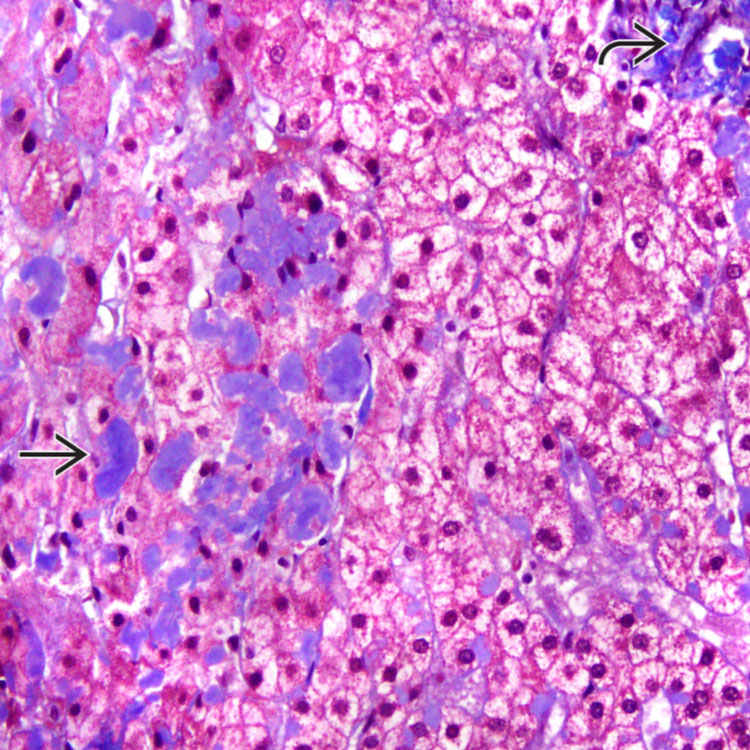
 stain with trichrome stain, but it is often a paler staining than that seen with collagen
stain with trichrome stain, but it is often a paler staining than that seen with collagen  .
.TERMINOLOGY
Definitions
• Heterogeneous disease characterized by deposition of glycoprotein fibrils in extracellular matrix and vessel walls

• Liver involvement may be seen in different types
 Primary, or AL, amyloidosis
Primary, or AL, amyloidosis




Primary, or AL, amyloidosis– Occurs alone or associated with other hematologic diseases (plasmacytoma, multiple myeloma Waldenstrom macroglobulinemia)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
