DRUG CLASSES
Sympathomimetics
Short-acting beta (β)-2 agonists
Long-acting β2 agonists
Optic agents (alpha 2 agonists/sympathomimetics)
PHARMACOLOGY IN PRACTICE

Janna Wong is brought into the clinic by her mother. Yesterday she was in the yard and came into the house crying after being stung by a bee. Later in the evening she complained of itching around her throat and what Janna called a “fat tongue.” As you read this chapter, think about what type of reaction this might have been.
The component of the peripheral nervous system (PNS) studied in this unit is a system of nerves that automatically regulates bodily functions—the autonomic nervous system. This system is further divided into the sympathetic and the parasympathetic nervous system branches. In this unit you will learn about the sympathetic branch, which is regulated by involuntary control. In other words, a person does not have control over what this system does. Activation of this branch is often called the fight-or-flight response. These nerves are activated when the body is confronted with stressful situations, such as danger, intense emotion, or severe illness. The sympathetic branch has control over a person’s heart rate, breathing rate, and ability to divert blood to the skeletal muscles—to enable a person to run, for example. Figure 24.1 illustrates how specific organs respond when the sympathetic branch is activated throughout the body.
Norepinephrine is a neurotransmitter produced naturally by the body. It is the primary neurotransmitter in the sympathetic branch of the autonomic nervous system and the substance that keeps the nerve message (or impulse) going from the brain to the target organ. Because this system is activated by the precursor of epinephrine (adrenalin), another term for the sympathetic pathway is the adrenergic branch. Therefore, the medicines used that work like the adrenergic branch are termed adrenergic drugs.
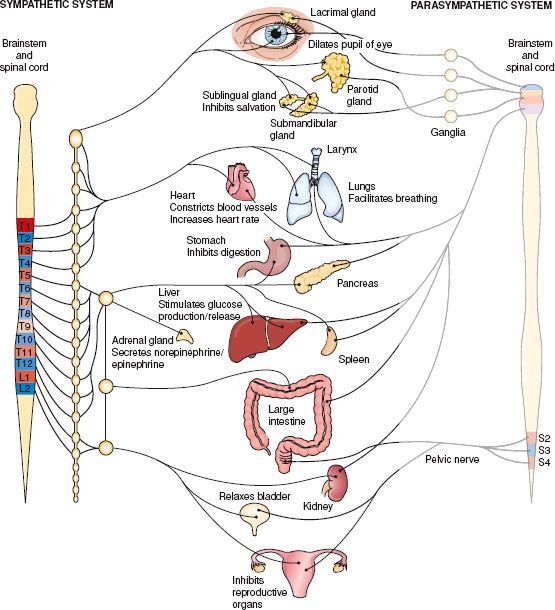
Figure 24.1 Action on body organs and structures when the sympathetic nervous system is stimulated. (Adapted from Cohen, B. J. [2003]. Medical terminology [4th ed.]. Philadelphia: Lippincott Williams & Wilkins.)
In the sympathetic branch of the autonomic nervous system, adrenergic drugs produce activity similar to the neurotransmitter norepinephrine. Another name for these drugs is sympathomimetic (i.e., mimicking the actions of the sympathetic nervous system) drugs. The adrenergic drugs produce pharmacologic effects similar to the effects that occur in the body when the sympathetic nerves (norepinephrine) and the medulla (epinephrine) are stimulated. The primary effects of these drugs occur on the heart, the blood vessels, and the smooth muscles, such as the bronchi of the lung.
Actions
The purpose of stimulating the sympathetic (adrenergic) nerves is to divert blood flow to the vital organs so that the body can deal with a stressful situation (the fight-or-flight response). In general, adrenergic drugs produce one or more of the following responses in varying degrees:
• Central nervous system—wakefulness, quick reaction to stimuli, quickened reflexes
• Autonomic nervous system—relaxation of the smooth muscles of the bronchi, constriction of blood vessels, sphincters of the stomach, dilation of coronary blood vessels, decrease in gastric motility
• Heart—increase in the heart rate
• Metabolism—increased use of glucose (sugar) and liberation of fatty acids from adipose tissue
Receptor Selectivity
The degree to which any organ is affected by the sympathetic nervous system depends on which postsynaptic nerve receptor sites are activated (Fig. 24.2). Adrenergic nerves have either alpha (α) or beta (β) receptors. Drugs that act on the receptors are called selective or nonselective. Adrenergic drugs may be selective (act on α receptors or β receptors only) or nonselective (act on both α and β receptors). For example, isoproterenol acts chiefly on β receptors; it is considered a selective drug. Epinephrine is a nonselective drug and acts on both α and β receptors.
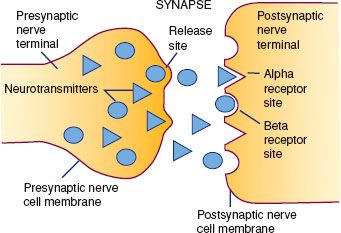
Figure 24.2 Neurotransmitter (e.g., norepinephrine), is released by the presynaptic nerve, crosses the synapse, and binds with α and β receptors in the cell membrane of the postsynaptic nerve, continuing the transmission of the nerve impulse.
Table 24.1 Effects of the Adrenergic Receptors
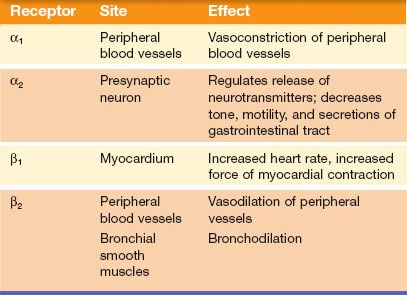
Whether an adrenergic drug acts on α, β, or α and β receptors accounts for the variation of responses to this group of drugs. Table 24.1 lists the type of adrenergic nerve receptor that corresponds with each action of the autonomic nervous system on the body. The α and β receptors can be further grouped as α1– and α2-adrenergic receptors and β1– and β2-adrenergic receptors.
Uses
Adrenergic drugs have a variety of uses and may be given for the treatment of the following:
• Hypovolemic and septic shock
• Moderate to severe episodes of hypotension
• Control of superficial bleeding during surgical and dental procedures of the mouth, nose, throat, and skin
• Cardiac decompensation and arrest
• Allergic reactions (anaphylactic shock, angioneurotic edema)
• Temporary treatment of heart block
• Ventricular arrhythmias (under certain conditions)
• Respiratory distress (as bronchodilators)
• Nasal congestion and glaucoma (topical formulation)
Patients at risk for life-threatening reactions to allergens, exercise, or unknown triggers may obtain and be instructed in the use of adrenergic drugs to lessen allergic reactions before emergency medical care is given.
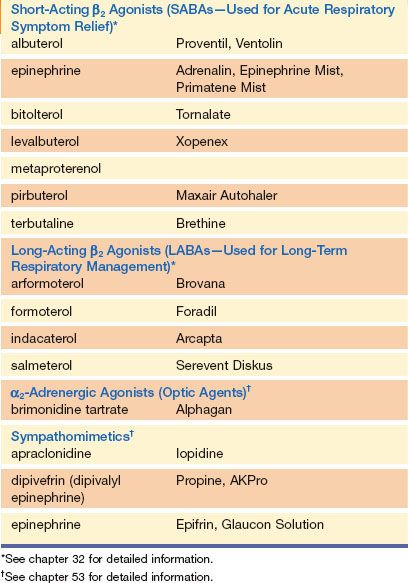
Adrenergic drugs may also be used as a vasoconstricting adjunct to local anesthetics to prolong anesthetic action in the tissues. The adrenergic drugs used primarily as vasopressors (drugs that raise the blood pressure because of their ability to constrict blood vessels) are listed in the Summary Drug Table: Adrenergic Drugs. Sympathomimetics are also used as bronchodilators in the treatment of respiratory problems (see Chapter 32) or topically in the treatment of glaucoma (see Chapter 53). These drugs are listed in Table 24.2 by name only; more information is provided in the respective chapters.
Table 24.2 Respiratory and Ophthalmic Sympathomimetics
Treating Shock
Adrenergic drugs are important in the care and treatment of patients in shock. Shock is a state of inadequate tissue perfusion. In shock, the supply of arterial blood and oxygen flowing to the cells and tissues is inadequate. To counteract the symptoms of shock, the body initiates physiologic mechanisms. The brain activates the hypothalamic-pituitary-adrenal (HPA) system. The HPA triggers the production of hormones and the release of epinephrine and norepinephrine. In some situations, the body is able to compensate, and blood pressure is maintained. However, if shock is untreated and compensatory mechanisms of the body fail, irreversible shock occurs and death follows. The three types of shock—hypovolemic shock, cardiogenic shock, and distributive shock—are described in Table 24.3.
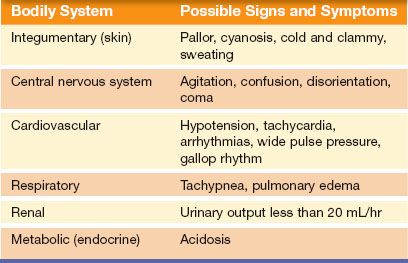
Various clinical manifestations may be present in a patient in shock. For example, in the early stages of shock, the extremities may be warm because vasodilation is initiated, and blood flow to the skin and extremities is maintained. If the condition is untreated, blood flow to the vital organs, skin, and extremities is compromised. The patient becomes cool and clammy, which is referred to as “cool” or “cold” shock. Regardless of the type, shock results in a decrease in cardiac output, decrease in arterial blood pressure (hypotension), reabsorption of water by the kidneys (causing a decrease in urinary output), decrease in the exchange of oxygen and carbon dioxide in the lungs, increase in carbon dioxide and decrease in oxygen in the blood, hypoxia (decreased oxygen reaching the cells), and increased concentration of intravascular fluid. This scenario compromises the functioning of vital organs such as the heart, brain, and kidneys. The various physiologic responses caused by shock are listed in Table 24.4.
Management of shock is aimed at providing basic life support (airway, breathing, and circulation) while attempting to correct the underlying cause. Antibiotics, inotropes, hormones (e.g., insulin, thyroid), and other drugs may be used to treat the underlying disease. However, the initial pharmacologic intervention is aimed at supporting the circulation with vasopressors.
Adrenergic drugs improve hemodynamic status by improving myocardial contractility and increasing heart rate, which results in increased cardiac output. Peripheral resistance is increased by vasoconstriction. In cardiogenic shock or advanced shock associated with low cardiac output, an adrenergic drug may be used with a vasodilating drug. A vasodilator, such as nitroprusside (see Chapter 35) or nitroglycerin (see Chapter 36), improves myocardial performance because the adrenergic drug maintains blood pressure.
Table 24.3 Types of Shock
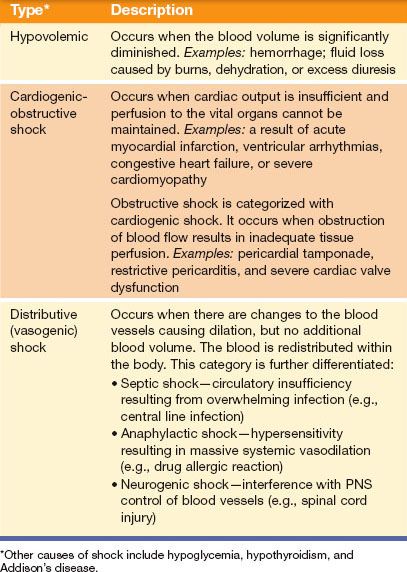
Table 24.4 Physiologic Manifestations of Shock
Adverse Reactions
Adverse reactions associated with the administration of adrenergic drugs depend on the drug used, the dose administered, and individualized patient response. Some common adverse reactions include:
• Cardiac arrhythmias (bradycardia and tachycardia)
• Headache
• Nausea and vomiting
• Increased blood pressure (which may reach dangerously high levels)
Additional adverse reactions for specific adrenergic drugs are listed in the Summary Drug Table: Adrenergic Drugs.
 LIFESPAN CONSIDERATIONS
LIFESPAN CONSIDERATIONS
Gerontology
The older adult is especially vulnerable to adverse reactions of adrenergic drugs, particularly epinephrine. In addition, older adults are more likely to have pre-existing cardiovascular disease that predisposes them to potentially serious cardiac arrhythmias. Closely monitor all older patients taking an adrenergic drug, and report any changes in the pulse rate or rhythm immediately. Also note, epinephrine may temporarily increase tremor and rigidity in older adults with Parkinson’s disease.
Contraindications
Adrenergic drugs are contraindicated in patients with known hypersensitivity. Isoproterenol is contraindicated in patients with tachyarrhythmias, tachycardia, or heart block caused by digitalis toxicity, ventricular arrhythmias, and angina pectoris. Dopamine is contraindicated in those with pheochromocytoma (adrenal gland tumor), unmanaged arrhythmias, and ventricular fibrillation. Epinephrine is contraindicated in patients with narrow-angle glaucoma and as a local anesthetic adjunct in fingers and toes. Norepinephrine is contraindicated in patients who are hypotensive from blood volume deficits. Midodrine causes severe hypertension in the patient who is lying down (supine).
 NURSING ALERT
NURSING ALERT
Supine hypertension is a potentially dangerous adverse reaction in the patient taking midodrine. The drug should be given only to patients whose lives are impaired despite standard treatment offered. This reaction is minimized by administering midodrine during the day while the patient is in an upright position. The suggested dosing schedule for the administration of midodrine is shortly before arising in the morning, midday, and late afternoon (not after 6:00 p.m.). Drug therapy should continue only in the patient whose orthostatic hypotension improves during the initial treatment.
Precautions
These drugs are used cautiously in patients with coronary insufficiency, cardiac arrhythmias, angina pectoris, diabetes, hyperthyroidism, occlusive vascular disease, or prostatic hypertrophy. Patients with diabetes may require an increased dosage of insulin. Adrenergic drugs are classified as pregnancy category C and are used with extreme caution during pregnancy.
Interactions
The following interactions may occur when an adrenergic drug is administered with another agent:
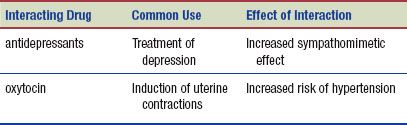
There is an increased risk of seizures, hypotension, and bradycardia when dopamine is administered with phenytoin (Dilantin). Metaraminol is used cautiously in patients taking digoxin because of an increased risk for cardiac arrhythmias. There is an increased risk of hypertension when dobutamine is administered with the β-adrenergic blocking drugs.
 HERBAL CONSIDERATIONS
HERBAL CONSIDERATIONS
Ephedra (Ma Huang) and the many substances of the Ephedra genus have been used medicinally (e.g., E. sinica and E. intermedia). Ephedra (ephedrine) preparations have traditionally been used to relieve cold symptoms and improve respiratory function, and as an adjunct in weight loss. Large doses may cause a variety of adverse reactions, such as hypertension and irregular heart rate. The use of ephedra has shifted from relief of respiratory problems to an aid to weight loss and enhanced athletic performance. Before taking this herb, the patient should consult a primary health care provider. Ephedra should not be used with the cardiac glycosides, halothane, guanethidine, monoamine oxidase inhibitor (MAOI) antidepressants, or oxytocin or by patients taking St. John’s wort. The U.S. Food and Drug Administration (FDA) warns the public not to take ephedrine-containing dietary supplements. Stroke and heart attack have resulted from taking these products. Many producers of weight loss supplements are removing the ephedra component because of potential legal liability (DerMarderosian, 2003).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


