VASCULAR TUMORS
Hemangiomas represent benign proliferations of blood vessels. They occur in both the superficial and deep soft tissues, as well as in the bone (Figure 12.1.1). Multiple hemangiomas are also elements of numerous syndromic conditions, including Maffucci and Klippel-Trenaunay syndromes. There are several different clinical and histologic subtypes; the most common forms are discussed separately in the following. All are benign lesions, but some can cause extensive morbidity.
CAPILLARY HEMANGIOMA
This represents the most common subtype of hemangioma and has a strong predilection for infants and children. They are occasionally present at birth. This form of hemangioma is also known by several other names including infantile hemangioma, juvenile capillary hemangioma, and lobular capillary hemangioma. This form of hemangioma initially presents with a rapid growth phase, often followed by a period of stabilization. Occasionally, a capillary hemangioma involutes spontaneously. They are frequently located on the face or in the oral mucosa. Most cases appear to be sporadic, although there is some speculation that there may be a rare familial capillary hemangioma syndrome.
Histologically, capillary hemangiomas are characterized by an intense cellular proliferation of small vessels, usually in the superficial subcutis and dermis (Figure 12.1.2). There are invariably some open capillaries with recognizable lumens, but the lesion may be so cellular that lumens are often focally absent (Figure 12.1.3). The endothelial cells tend to be small and monomorphic, although mitotic activity can be brisk. Mast cells are a common finding in the more proliferative stage of capillary hemangioma.
By immunohistochemistry, the endothelial cells stain for the erythrocyte-type glucose transporter protein GLUT1 (Figure 12.1.4). This is an important marker in that it helps distinguish this variant of hemangioma from other vascular lesions. Capillary hemangiomas often respond well to nonsurgical treatments including topical or intralesional steroids as well as the beta-blocker propranolol. In addition, capillary hemangiomas often spontaneously involute, whereas other types of hemangioma are less likely to do so.
CAVERNOUS HEMANGIOMA
Cavernous hemangiomas occur in both children and adults. They may be cutaneous or deep seated, occurring commonly in the liver, lung, bone, and gastrointestinal tract. These are sometimes also called venous hemangiomas or venous malformations. Cavernous hemangiomas may be one feature of a number of multiorgan diseases including Maffucci and Klippel-Trenaunay, and blue rubber bleb syndromes.
Cavernous hemangiomas are characterized by large ectatic vascular channels lined by flattened endothelium (Figure 12.1.5). A variant of cavernous hemangioma is the so-called “hobnail” or targetoid subtype. The “targetoid” description refers to the clinical appearance of the lesion (Figure 12.1.6). Venous hemangiomas differ slightly from cavernous hemangiomas in that the vessel walls may show variable thickness.
EPITHELIOID HEMANGIOMA
Epithelioid hemangioma is sometimes also referred to as angiolymphoid hyperplasia with eosinophilia. This is an uncommon lesion, which tends to occur in young to middle-aged adults. It may be superficially located within the dermis or more deep seated in bone and soft tissues. Interestingly, about 20% of patients present with multiple lesions. In addition, a small percentage of patients have peripheral blood eosinophilia and/or lymphadenopathy.
The epithelioid variant of hemangioma closely resembles an epithelial lesion and can occasionally be confused with carcinoma. It typically has a lobular configuration with a proliferation of plump, cuboidal to epithelioid cells with abundant cytoplasm. As with other variants of hemangioma, this lesion may be so cellular that malignant entities, including both carcinoma and angiosarcoma, are often entertained in the differential diagnosis. The cells tend to form cord-and gland-like spaces, often within a myxoid-appearing background. A variable histologic feature is the presence of an extensive inflammatory infiltrate, often with a predominance of eosinophils (Figure 12.1.7).
GLOMERULOID HEMANGIOMA
Glomeruloid hemangiomas are an extremely rare variant of benign vascular neoplasm, most often identified in association with POEMS syndrome (Polyneuropathy, Organomegaly, Endocrinopathy or Edema, M-protein, and Skin manifestations such as hyperpigmentation or hypertrichosis). POEMS tends to occur in older adults, with average age of onset around 50 years. Of note, patients with POEMS can have other vascular lesions aside from glomeruloid hemangioma.
Glomeruloid hemangiomas are most often located in the dermis and tend to occur on the trunk and proximal extremities. Histologically, these are complex intravascular proliferations that resemble the normal glomerulus of the kidney (Figure 12.1.8). They are comprised of small ectatic vessels with small lumens. The endothelial lining may be flat or can have a vacuolated appearance. One very characteristic feature is the presence of hyaline globules both within the endothelial cytoplasm and within the stromal cells (Figure 12.1.9). The hyaline material has a proteinaceous appearance and represents immunoglobulin.
SYNOVIAL HEMANGIOMA
This lesion is defined by its location within the synovium. Children and young adults are most commonly affected. The most common site is within the knee joint. Patients present with pain and swelling of the affected region, often of long duration.
Histologically, synovial hemangiomas show variable histologic features. The vascular component may include small capillary and larger venous-type vessels in addition to an arterial component (Figure 12.1.10). Degenerative changes, including hemosiderin deposition, focal infarction, and intravascular fibrin deposition, are often present.
PAPILLARY ENDOTHELIAL HYPERPLASIA (MASSON TUMOR)
Although not a true hemangioma, Masson tumor is often included in the discussion of hemangioma because of its histologic similarity to other vascular tumors. This is a benign condition that represents a florid endothelial proliferation within an organizing thrombus. Keys to its benign nature include its circumscription and confinement to a vessel (Figures 12.1.11 and 12.1.12).

FIGURE 12.1.1 Phleboliths developing within a longstanding hemangioma of the soft tissues of the distal upper extremity.
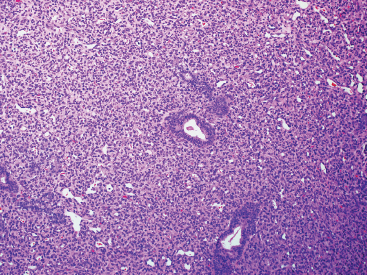
FIGURE 12.1.2 Juvenile forms of hemangioma are frequently very cellular. In this example, the cellular proliferation has infiltrated around the adnexal structures of the dermis.
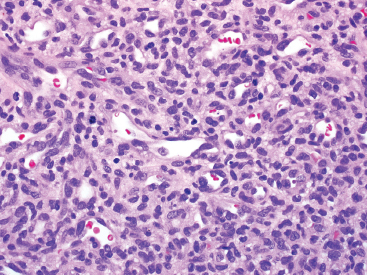
FIGURE 12.1.3 On higher power, small lumens are identified within the vascular proliferation. Despite the overall cellularity, the nuclei appear fairly monomorphic. Note also the mitotic activity within the lesion.
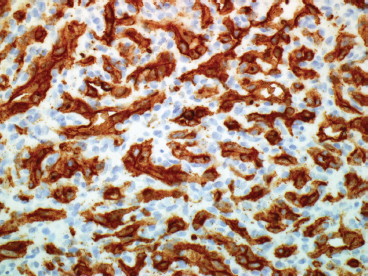
FIGURE 12.1.4 Immunohistochemical staining for GLUT1 distinguishes the juvenile or cellular variant of capillary hemangioma from other lesions. This distinction is important for potential therapeutic decision making.
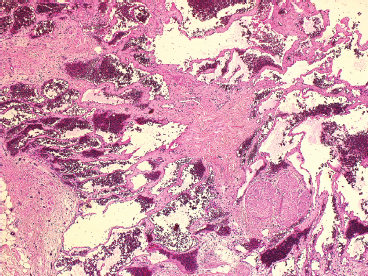
FIGURE 12.1.5 Cavernous types of hemangioma are often located within the superficial or deep soft tissues as well as bone.
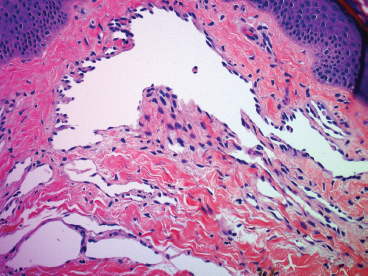
FIGURE 12.1.6 Some cavernous types of hemangiomas display a slight “hobnail” appearance to the endothelial lining. This should not be mistaken for a more aggressive neoplasm.
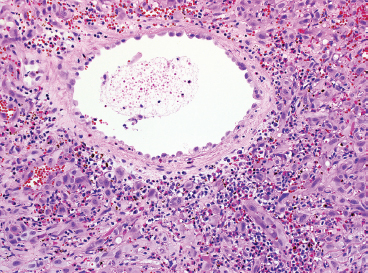
FIGURE 12.1.7 An epithelioid hemangioma centered on a larger vessel. This proliferation is accompanied by an inflammatory infiltrate composed of mononuclear cells and eosinophils. In this setting, this lesion is sometimes referred to as angiolymphoid hyperplasia with eosinophilia.
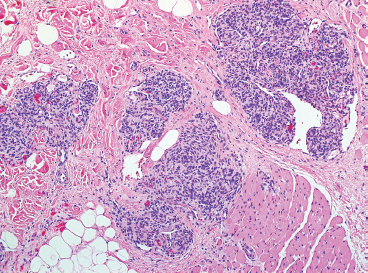
FIGURE 12.1.8 Glomeruloid hemangioma composed of small glomerulus-like proliferations in the deep dermis.
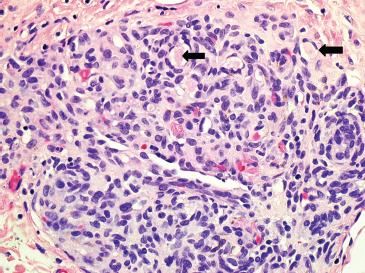
FIGURE 12.1.9 Glomeruloid hemangiomas typically have small hyaline droplets of immunoglobulin (arrows).
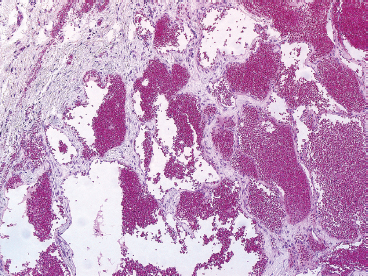
FIGURE 12.1.10 Hemangiomas of the synovium are usually cavernous in appearance. They can cause joint swelling and effusion.
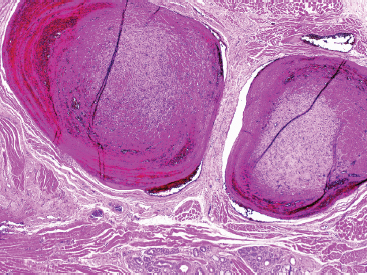
FIGURE 12.1.11 Papillary endothelial hyperplasia (Masson tumor) on low power. These can cause swelling or nodular masses, particularly on the hands and fingers.
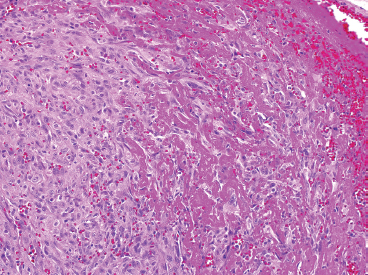
FIGURE 12.1.12 At higher power, it is more obvious that this lesion represents an organizing thrombus rather than a true vascular neoplasm.
Hemangioendotheliomas represent a diverse subset of vascular neoplasms of intermediate-grade potential. They are usually locally aggressive and tend to recur, but rarely metastasize. Patient age and location of the lesion are dependent on the subtype of tumor. Kaposiform hemangioendothelioma, for example, occurs in young children and infants and has a predilection for the retroperitoneum. Composite-type hemangioendothelioma tends to occur on the extremities of adults. These two variants, as well as retiform hemangioendothelioma, represent very rare subtypes of tumor.
The vast majority of hemangioendotheliomas are of either a spindle cell or an “epithelioid” subtype. Epithelioid hemangioendothelioma (EHE) can occur in both children and adults, and affects both sexes equally. It occurs in superficial and deep soft tissue as well as bone. EHE also occurs in the liver and lung. EHE can also be multicentric, with combinations of soft tissue, liver, lung, and bone lesions. EHE is associated with a significant risk of recurrence and metastasis, estimated to occur in up to 25% of cases. Interestingly, EHE is one of the few soft tissue tumors that tends to metastasize to lymph nodes. Because EHE is a potentially aggressive neoplasm, treatment strategies include a wide local resection wherever possible as well as adjuvant therapy in selected cases.
EHE is characterized by a reproducible chromosomal translocation t(1;3)(p36;q23-25) that can be useful in confirming the presence of this lesion in diagnostically challenging cases.
HISTOPATHOLOGY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


