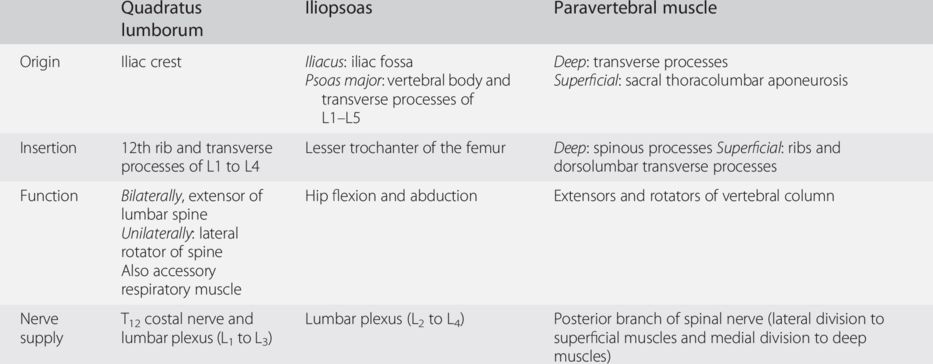
Quadratus lumborum muscle
Dysfunction of the quadratus lumborum muscle is considered the most common cause of low-back pain by many authors (Travell and Simmons, 1983). Its impairment may be severely disabling as it plays an important stabilizing role in the spine, and makes the load of standing body weight intolerable.
Review of anatomy
The quadratus lumborum muscle is found on the posterolateral aspect of the lumbar spine and has a flat, quadrilateral morphology. It inserts below the outer border of the iliac crest, above the lower border of the 12th rib and in its medial portion on the tips of the transverse processes of L1–L5 (Fig. 29.1). It is formed by fibers that cross one another in three directions:
- costotransverse fibers stretch from the transverse processes of L1 to rib 12
- iliotransverse fibers run from the iliac crest to the transverse processes of the last four lumbar vertebrae
- iliocostal fibers extend from the iliac crest to the lower border of rib 12.
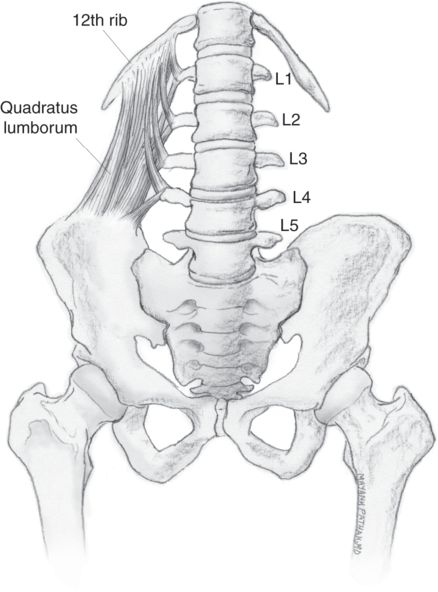
Fig. 29.1 Anterior view showing the insertion sites of the quadratus lumborum muscle.
When the subject is erect, the muscle acts to stabilize the lumbar spine on the pelvis. Unilateral contraction flexes the lumbar spine to the same side. With the spine fixed, the muscles’ function is to elevate the hip on the same side. Bilateral contraction allows extension of the lumbar spine and trunk. It is also an accessory respiratory muscle.
The nerve supply for the quadratus lumborum muscle is provided by thoracic nerve T12 and the lumbar plexus (L1 to L3 spinal nerves).
Symptoms
Pain is reported by patients as deep and worsens with standing or unsupported sitting. The typical pain distribution caused by quadratus lumborum muscle dysfunction is depicted in Fig. 29.2.
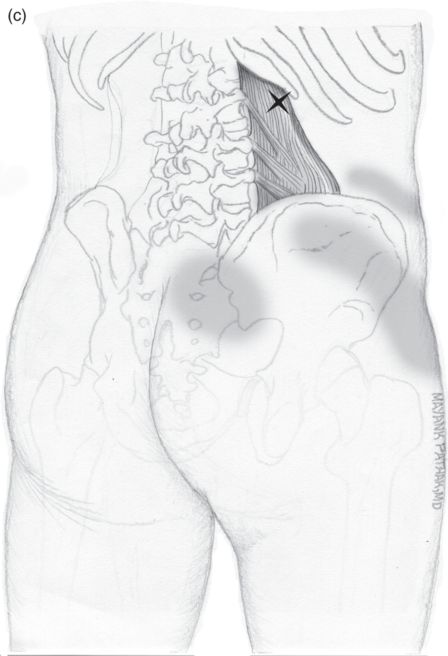
Fig. 29.2 Patterns of referred pain of the trigger points of the quadratus lumborum muscle. (a,b) Pain pattern of superficial trigger points, palpable below and next to the 12th rib (a) and above the iliac crest (b). (c) Pain pattern of deep trigger points next to the lumbar transverse processes.
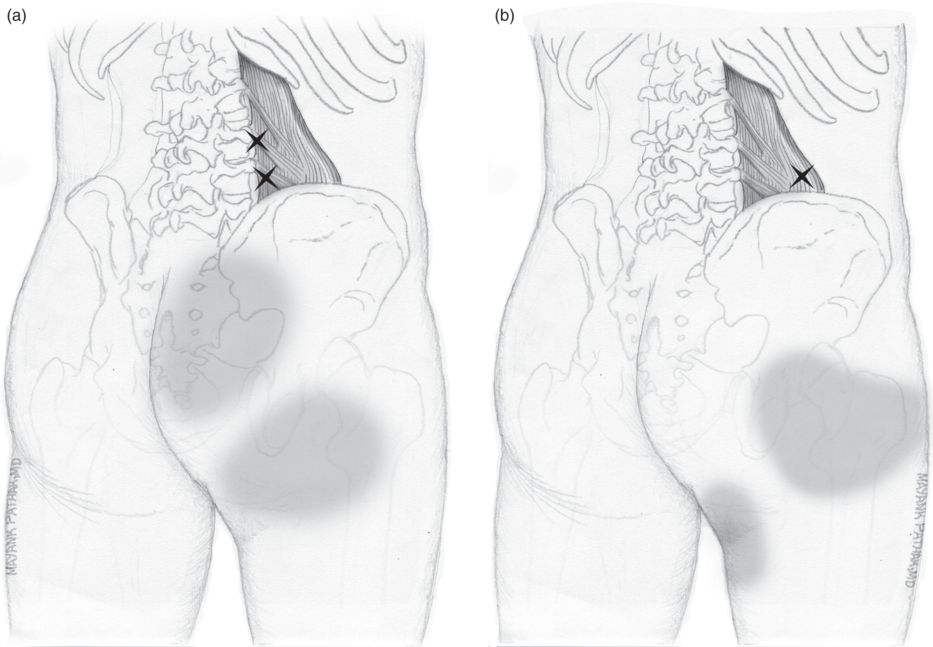
Typically, pain may extend to the groin and genital areas and sometimes simulate a distribution compatible with sciatic nerve dysfunction, with referred pain over the area of the sacroiliac joints and lower buttocks.
The upper trigger points show a typical pattern of pain toward the sacroiliac joints and trochanteric region. The lower trigger points radiate toward the buttocks. It is important in these cases to consider differential diagnosis with pain originating in the lumbar zygapophyseal joints and pain from nerve root involvement (particularly S1), which may show similar patterns of pain radiation. The severity of pain may become completely disabling for the patient.
Patients have difficulty in flexing the trunk, rotating it to the contralateral side of the affected side or leaning toward any position when lying in a supine position. They may also report difficulty in rising from a sitting position without using the arms. In acute cases, coughing or sneezing may be painful.
Examination
An examination should be performed for rotation and lateral flexion mobility of the lumbar spine; both will be painful, but lateral flexion will be the most affected. Contracture of the quadratus lumborum may cause a functional lumbar scoliosis of convexity contralateral to the affected side as well as declination of the contralateral hemipelvis (Travell and Simmons, 1983).
For examination of the trigger points, the patient is placed in lateral decubitus position on the contralateral side. With patient in this position, a rolled sheet is placed in the lower part of the lumbar spine, leaving the upper leg behind the other until the knee touches the table; the upper arm is extended above the head to grip the edge of the table, so that the space between the last rib and the iliac crest is opened to the maximum, permitting optimal access to the muscle (Fig. 29.3). In this position, trigger points are examined by pressing down on the areas next to the iliac crest and the 12th rib (superficial trigger points), which causes pain that radiates to the trochanter, and external side of the thigh and in the area next to the lumbar spine, which causes pain that radiates to the sacroiliac joints and buttocks.
Fig. 29.3 Patient position to examine the quadratus lumborum muscle. Complete opening of the iliocostal space is achieved by placing a pillow below the lumbar spine and making the upper knee rest on the table behind the lower leg. Illustrated by Mayank Pathak, redrawn from author’s original.
Treatment
The doses of the different types of BoNT used for treatment of quadratus lumborum muscle dysfunction are summarized in Table 29.2.

The technique to infiltrate the quadratus lumborum muscle is classically performed under X-ray guidance. With the patient in a prone position, the X-ray unit is placed in anteroposterior projection and the highest point of the iliac crest is located. The space between the spinal processes of L4 and L5 is located and a mark is made on the skin above the highest point of the crest at the height of the L4–L5 space (Fig. 29.4a).
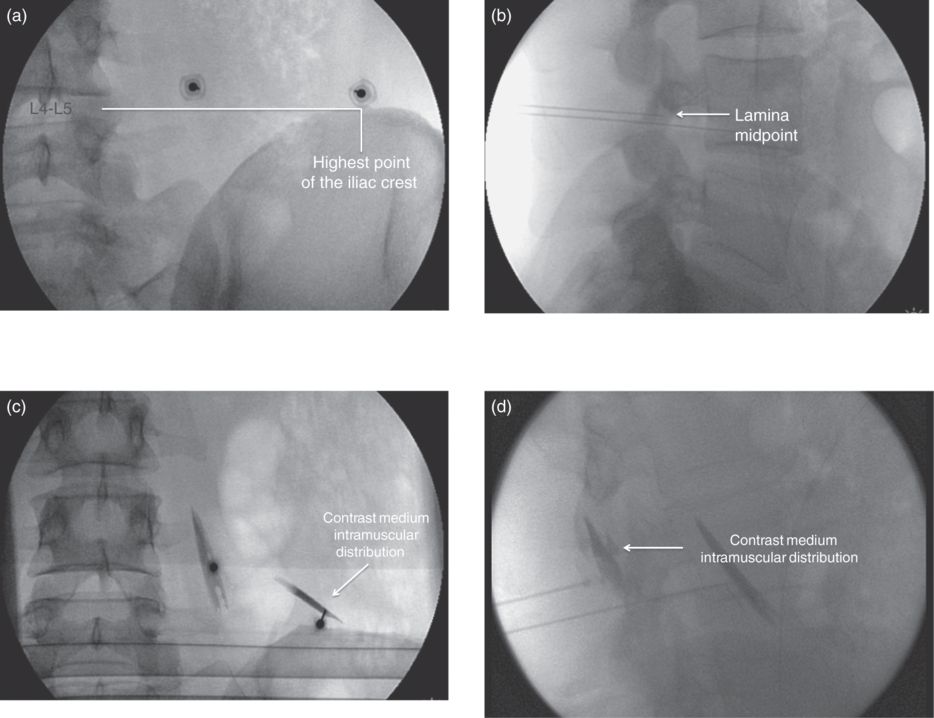
Fig. 29.4 Infiltration of the quadratus lumborum muscle under X-ray guidance. (a) Anteroposterior image showing the references for quadratus lumborum muscle puncture. The highest point of the iliac crest is located and the space between the transverse processes L4 and L5. (b) Lateral image showing the references for quadratus lumborum muscle puncture. The needle has been advanced to the point where it is in the midpoint of the lamina of the corresponding vertebra. (c) Anteroposterior view with iodine contrast, showing intramuscular distribution. (d) Lateral view with iodine contrast, showing intramuscular distribution.
The skin is infiltrated with a small amount of local anesthetic using a Quincke-type, 22-gauge, 90 mm spinal needle inserted perpendicular to the skin.
Once the needle is firmly secured and tunnel vision is obtained, the X-ray unit is placed in lateral view, and the needle is advanced in this projection until it reaches the midpoint of the lamina of the corresponding vertebra (Fig. 29.4b).
The X-ray is placed again in anteroposterior projection and 0.2 ml of water-soluble contrast medium is injected, and an image of intramuscular distribution should be obtained in anteroposterior (Fig. 29.4c) and lateral (Fig. 29.4d) view. Once the image is obtained, injection of BoNT is performed.
This procedure has also been described using ultrasound guidance (Curatolo and Eichenberger, 2007).
The main risk when performing infiltration of the quadratus lumborum muscle is penetrating into the abdominal cavity with the needle or causing damage to structures such as the kidneys since this muscle is one of the muscles making up the posterior abdominal wall (Fig. 29.5).
Fig. 29.5 Anatomical section at the level of L2. When accessing the quadratus lumborum muscle, the greatest risk is penetration of the abdominal cavity or injury to the renal poles.
Iliopsoas muscle
Review of anatomy
The psoas major muscle is inserted proximally on the sides of the vertebral bodies of the last thoracic vertebra and all the lumbar vertebrae, as well as in the anterior borders and lower surfaces of the lumbar transverse processes. Hence it is situated next to the vertebral bodies and in front of the transverse processes (Fig. 29.6).
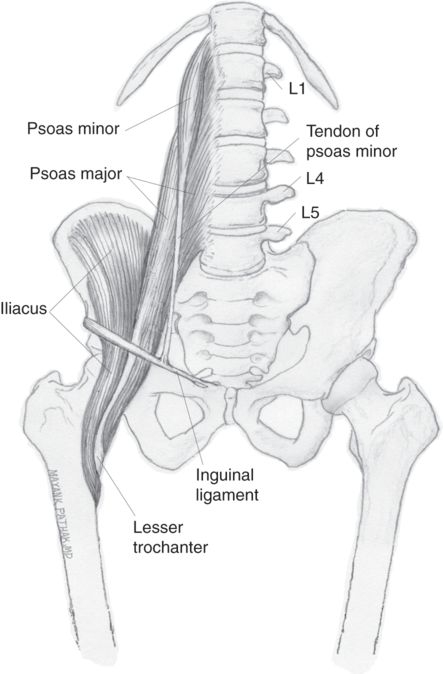
Fig. 29.6 Insertion sites of psoas major, iliac and psoas minor muscles.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


