| Excessive writers | Musicians | Others |
|---|---|---|
| Students | Pianists | Typists |
| Teachers | Horn player | Telegraphers |
| Clerks | Clarinetists Guitarists Violinists Flutists Saxophonists | Computer operators Watch makers Seamstresses Surgeons/dentists Golfers Fencing masters Cobblers Tailors Bookmakers |
This chapter discusses writer’s cramp and musician’s dystonia (cramp) in detail, the two most common occupational dystonias, followed by a discussion of other focal occupational dystonias.
Pathogenesis
The exact cause of FHD is not yet elucidated. A consistent physiological finding is excessive activation of antagonists and overflow and prolongation of muscle activation. Both of these are thought to reflect deficiency of inhibition at multiple levels of the motor system circuitry (Hallett, 2000, 2006a,b). Dopamine dysfunction has also been implicated. Although FHD is a movement disorder, somatosensory dysfunction is also present, including distorted sensory maps of the affected hand (Bara-Jimenez et al., 1998) and impaired sensory discrimination (Sanger et al., 2001). Structural MRI analyses have shown increased gray matter volume in the basal ganglia of musicians (Granert et al., 2011) and writers (Garraux et al., 2004) with FHD. Functional MRI has shown impaired activation of the primary sensorimotor and supplementary motor cortex during voluntary muscle relaxation and contraction (Oga et al., 2002). A genetic factor in the development of hand dystonia is possible, as up to 20% of patients with writer’s cramp have family members with dystonia.
As with other focal dystonias, it is likely that FHD arises from an interaction of proprioceptive, behavioral, genetic, environmental and psychological factors. Hand overuse or repetitive motions using small hand muscles may be a precipitating factor, particularly in the presence of a putative underlying genetic predisposition (Hallett, 1998).
Writer’s cramp
Writer’s cramp was first reported amongst scribes in the eighteenth century under the term “occupational palsy,” where some workers had disabling spasms of their hands only when performing their jobs (Ramazzini, 1713; Solly, 1864). This task-specific FHD may be particularly likely in people whose profession involves excessive writing. The incidence of writer’s cramp has been reported at 14 per million in Europe (Epidemiological Study of Dystonia in Europe, 2000) and 2.7 per million in Rochester Minnesota (Nutt et al., 1988). These figures may be underestimates, as suggested by a recent population-based study that found writer’s cramp to be the most common focal dystonia (Das et al., 2007). Among the various forms of focal dystonias, writer’s cramp is variably reported to be seen in 5% to 19% of cases (Duffey et al., 1998; Epidemiological Study of Dystonia in Europe, 2000). In contrast to other focal dystonias, writer’s cramp is seen more frequently in men than in women (Soland et al., 1996; Duffey et al., 1998; Epidemiological Study of Dystonia in Europe, 1999).
Clinical subtypes
In “simple writer’s cramp,” acts requiring dexterity other than writing, such as buttoning clothes or handling of forks and knives, are unimpaired. Some patients have dystonia elicited by tasks other than writing as well and are said to have “dystonic writer’s cramp,” but the term “complex writer’s cramp” may be more appropriate (Jedynak et al., 2001). Simple writer’s cramp can be a prelude to complex writer’s cramp, but for many patients the condition remains simple. When severe, dystonic posturing may be present at rest as well as during eliciting tasks.
Dystonic posturing is more often flexor than extensor and can involve the wrist and arm as well as the fingers. Less commonly, there is a combination of flexion and extension in the same hand. Uncontrolled pronation or supination may also be present. Arm abduction may occur while writing, which could be a primary component of the dystonia or a compensatory mechanism (Fig. 10.1).
Fig. 10.1 Arm abduction pattern. Arm abduction while writing may be dystonic or compensatory.
Disability in writer’s cramp
When writing, dystonic muscle activity interferes with normal muscle activation patterns. Not infrequently, muscle aching develops, largely as a consequence of the excessive muscle contractions. The severity of pain usually does not correlate with the severity of writing impairment but may correlate with the handicap score (Jedynak et al., 2001).
In contrast to disability during writing, patients with writer’s cramp are often able to conduct most of their other activities without difficulty. In other tasks requiring activation of the same muscle groups, the hand appears normal and performs unremarkably. Such task specificity is a characteristic feature of writer’s cramp and other FHDs.
Frequently patients switch to writing with the non-dominant hand. Unfortunately, writer’s cramp tends to develop in the non-dominant hand in 10–15% of the patients. About half of the patients with writer’s cramp have “mirror dystonia,” with dystonic muscle activity elicited in their dystonic hand when they write with the non-dystonic hand (Jedynak et al., 2001). Occasionally, writer’s cramp is associated with other focal dystonias, such as cervical dystonia or oromandibular dystonia. Almost half of those with writer’s cramp have postural tremor in the affected hand (Rosenbaum and Jankovic, 1988).
Musician’s dystonia
Musician’s dystonia (cramp) is the term applied to a focal dystonia localized to hand muscles controlling fine movements of the digits or the embouchure muscles involved in playing instruments (Tubiana, 2003). Similar to writer’s cramp, musician’s FHD can be task specific, with abnormal spasms or posturing of isolated muscle groups apparent only during playing. Musicians affected with FHD report lack of coordination while playing that is frequently accompanied by involuntary flexion or extension of fingers, particularly during music passages that emphasize rapid and forceful finger movements (Wilson et al., 1993).
In pianists, the fingers most often implicated are the two ulnar digits. These two fingers constitute the power grip part of the hand; they are not designed for the prolonged, rapid, highly complex movements demanded in musical performance (Newmark and Hochberg, 1987). However, the radial digits and thumb may also be involved, particularly the thumb of the right hand in pianists. In violinists and viola players, the left, non-bowing, hand is more frequently involved. In wind players, the hand supporting the instrument and doing the fingering at the same time is most often affected (e.g. left hand in flutists and right hand in clarinetists) (Fig. 10.2).
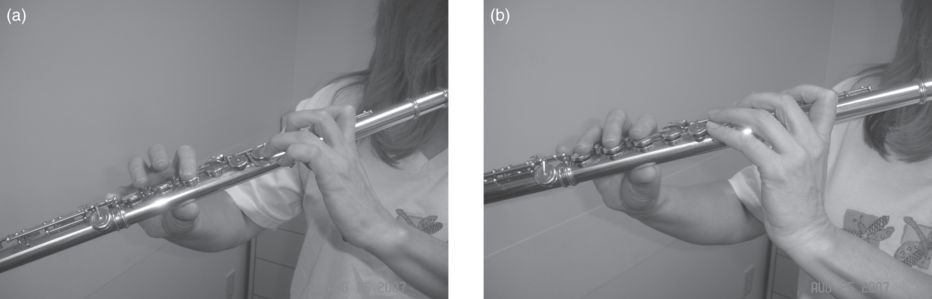
Fig. 10.2 Musician’s dystonia. (a) dystonic flexion in the left second, third and fourth fingers and wrist. (b) Non-dystonic hand posture: the hand is relaxed with slight curving of the fingers and the wrist.
Sometimes the onset of symptoms is found to coincide with a period of intense musical activity and overuse, such as preparation for a competition or obsessive practice in an attempt to increase the speed of a difficult passage. Usually the disorder does not progress beyond the focal task-specific problem, although it sometimes generalizes to other tasks or other parts of the body. The examination of the patient while playing the instrument that elicits the dystonia is important for the diagnosis and to target therapy.
Treatment of writer’s cramp
Non-pharmacologic approaches may have some utility in the treatment of FHD. Physical therapy or splints are sometimes helpful. Various pens, such as those with thicker barrels or that place the hand in a different position, may decrease fatigue and enable clearer writing in some patients. Sensory training to try to restore a more normal pattern of sensory representation has been tried. For example, learning Braille reading and practicing for 30–60 minutes per day for up to 1 year has provided some benefit (Zeuner et al., 2002; Zeuner and Hallett, 2003) as well as specific types of motor training (Zeuner et al., 2005). Limb immobilization via a plastic splint for 4–5 weeks has been proposed, but the value of this has been questioned and would not be recommended. Stereotactic nucleus ventrooralis thalamotomy has shown benefit for up to 29 months in writer’s cramp (Taira et al., 2003) and deep brain stimulation is being explored (Cho et al., 2009), but these should be considered experimental at this time. Oral medications, such as trihexyphenidyl or clonazepam play a limited role in the treatment of FHD.
Botulinum neurotoxin therapy
Injection of botulinum neurotoxin (BoNT) has been shown to be safe and effective in the treatment of FHD (Simpson et al., 2008). The first step in using BoNT to treat hand dystonia is careful evaluation and selection of muscles for injection. The patient should be examined at rest and during movements that specifically activate the dystonia: writers should be observed while writing and musicians while playing their instruments. However, the complexity of such movements often makes it difficult to determine which movements are dystonic, which are parts of the normal pattern for that activity and which are compensatory. Patients with writer’s cramp should be asked to write without trying to compensate and to describe any abnormal pulling that they experience. It is often helpful also to have the patient perform other activities that may elicit the dystonia without associated movements or compensation. Writing with the non-dominant hand, which can evoke dystonia in the dominant, resting hand (mirror dystonia), is one such strategy. Mirror dystonia can be helpful to identify dystonic muscle activity and to distinguish dystonia from compensatory muscle activity (Singer et al., 2005). The efficacy of treatment depends critically on the correct choice of muscles for injection.
Botulinum neurotoxin is effective in writer’s cramp and other occupational dystonias (Karp et al., 1994; Karp, 2004). The onset of benefit starts approximately 1 week after injection, peaks at 2 weeks and lasts approximately 3 months. Benefit can be demonstrated objectively as well as subjectively. A quantitative analysis by Wissell et al. (1996) using the Writer’s Cramp Rating Scale performed on 31 patients showed a good response to BoNT. The mean dose injected per session was 133.2 U abobotulinumtoxinA. Of all 124 injection sessions during a mean follow-up of 1 year, 76% produced a good improvement. The most common side effect was weakness with 72% of the injection sessions. The scores on the Writer’s Cramp Rating Scale and the speed of the pen movements showed significant improvement after treatment. Other studies have shown more than half of the patients with writer’s cramp returned repeatedly and could have sustained benefit for long follow-up periods (Turjanski et al., 1996; Hsuing et al., 2002; Lungu et al., 2011).
In a study of 53 patients by Karp et al. (1994), patients with localized writer’s cramp fared better and those with associated tremors fared the worst. In a prospective study on 47 patients, Djebbari et al. (2004) showed that those with a flexion and pronation of the forearm and those with thumb extension have a significantly better response on the Burke–Fahn–Marsden Scale. An earlier placebo-controlled double-blind study by Tsui et al. (1993) also showed better outcome in those with wrist deviation. The restoration of normal motor function in focal task-specific dystonias may be better when treatment is initiated as early as possible and when motor performance deterioration is still mild.
Injection sites are generally chosen based on clinical observation of muscle spasm during the precipitating task, perhaps supplemented with observations of mirror dystonia. The injections are most often given into muscle localization points described in manuals of electromyography (EMG) using specialized EMG/injection needles, so that EMG can be used to ensure that the needle is in the proper muscle. The intended muscle or fascicle may be missed in up to 50% of attempts to place the needle in a forearm muscle without use of EMG (Molloy et al., 2002). Use of EMG for guidance is particularly recommended where deeper muscles are targeted. Ultrasound can also be a valuable tool for accurate targeting. Injection of BoNT is into one, two or more sites depending on the dose to be injected and the muscle bulk. Data are available on the safety and efficacy of onabotulinumtoxinA and abobotulinumtoxinA for FHD. There have been no FHD studies reported with rimabotulinumtoxinB or incobotulinumtoxinA and there have been no trials directly comparing the efficacy of the different commercially available formulations of BoNT in writer’s cramp.
Commonly injected muscles and patterns
Treatment with BoNT relies on recognizing which muscles contribute to different patterns of dystonic movement and a thorough knowledge of arm and hand anatomy.
Focal flexor pattern
In the focal flexor pattern (Fig. 10.3), the thumb and/or the index finger flexes with writing. The flexor pollicis longus and/or brevis are involved in the thumb flexion. Individual fascicles of the flexor digitorum superficialis or profundus can also be involved and are associated with proximal or distal finger flexion, respectively.
Fig. 10.3 Focal flexor pattern.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


