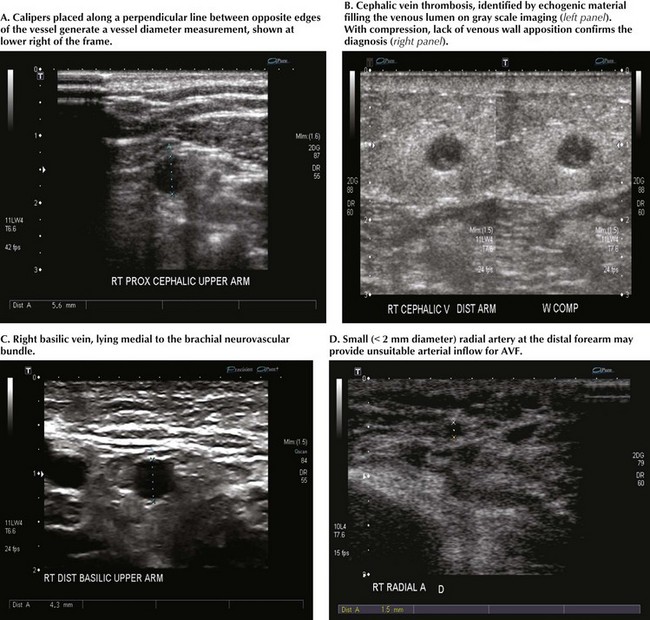
Chapter 35 Standard vessel-mapping protocols provide important information regarding approach to the best AVF or AVG location. Cephalic vein diameter is shown in Figure 35-1, A. Venous fibrosis, identified by thickened vein walls or incomplete compressibility, may predict poor distensibility with arterial inflow. Thrombosis from venipuncture or IV placement is shown in gray-scale imaging (Fig. 35-1, B). The basilic vein often lies deep and medial in the arm and will need superficialization if used for AVF (Fig. 35-1, C). A small or heavily calcified radial artery at the wrist, a common finding in diabetic patients, may contraindicate use of this artery for inflow (Fig. 35-1, D).
Upper Extremity Arteriovenous Access for Hemodialysis
Preoperative Evaluation
Preoperative Vessel Mapping by Duplex Ultrasound
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Upper Extremity Arteriovenous Access for Hemodialysis