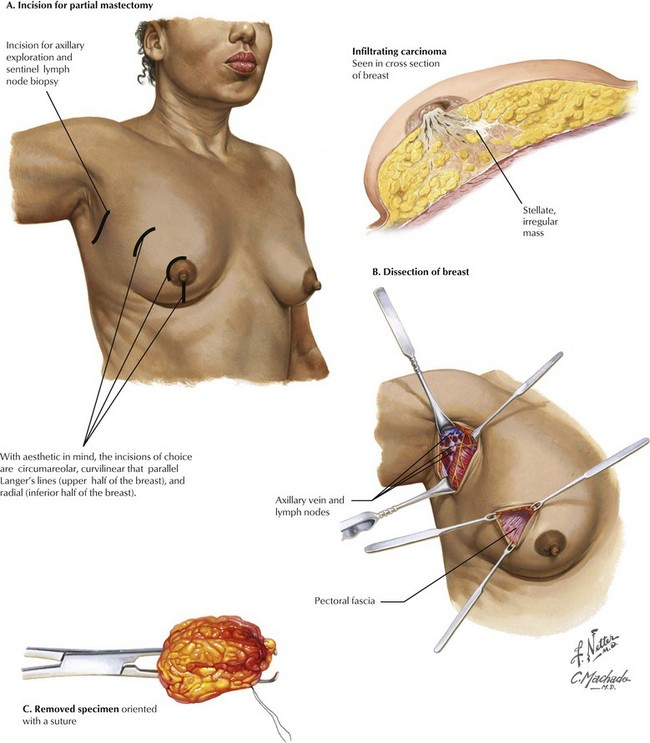
Chapter 46 With breast conservation and aesthetics the focus of partial mastectomy, the choice of incision is of great importance (Fig. 46-1, A). Circumareolar incisions provide good cosmesis. Curvilinear incisions that parallel Langer’s lines of tension in the upper half of the breast also work well. In the inferior half of the breast, radial incisions provide good cosmesis. For palpable lesions, the incision should be made directly over the tumor. For nonpalpable tumors localized with a wire, care should be made to make the incision over the expected location of the tumor and not necessarily at the insertion of the wire. Small skin flaps are raised, and then dissection can be performed sharply or with electrocautery. Breast tissue can be grasped with an Allis forceps to facilitate dissection, but care should be used to avoid tearing the tissues (Fig. 46-1, B). Although currently no consensus exists on margins to obtain for breast-conserving surgery, it is important that the entire lesion is removed with negative margins. Once removed, the specimen must be oriented so that if a margin is positive, another more localized excision can be done (Fig. 46-1, C).
Mastectomy
Partial Mastectomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


