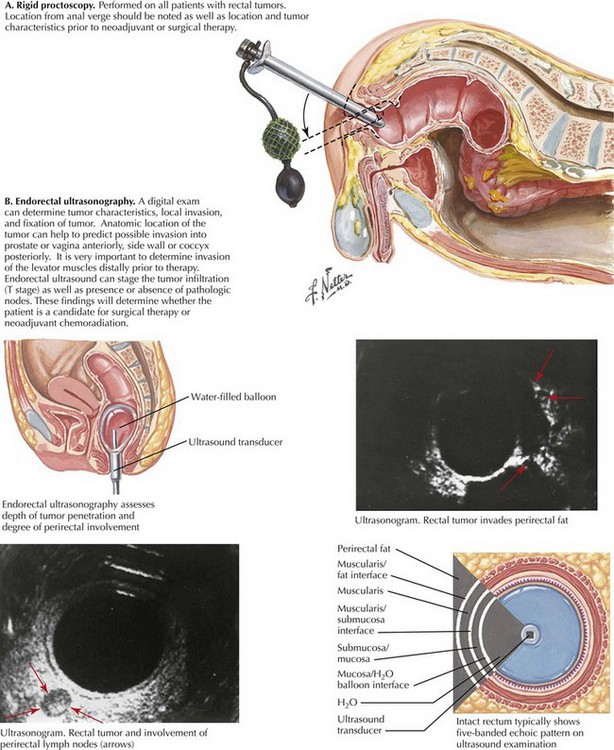
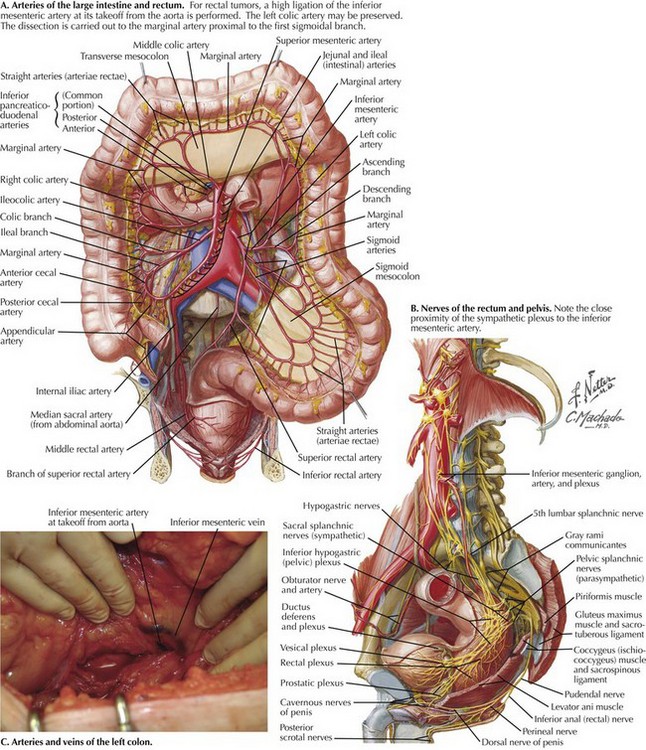
Chapter 25 The patient is screened with a full colonoscopy. Digital rectal examination and proctoscopy are performed to confirm tumor location and to assess feasibility of a sphincter-sparing approach (Fig. 25-1, A). Digital vaginal examination and vaginoscopy are performed with the proctoscope to assess for local invasion. CT scanning of the chest, abdomen, and pelvis is done to survey for metastatic disease. Endorectal ultrasound is used for staging to assess the need for preoperative chemoradiation (Fig. 25-1, B). The mobilization is extended to the root of the mesentery, and the inferior mesenteric artery is identified at its takeoff from the aorta (Fig. 25-2, A). Branches of the sympathetic nerves, which lie deep to the IMA, are protected by keeping close to the fascia of the mesocolon as it wraps around the IMA, if necessary sweeping nerve branches dorsally and away from the vessel (Fig. 25-2, B). The IMA is isolated, clamped, and ligated. The left colic artery and the inferior mesenteric vein are divided and ligated at the level of the IMA (Fig. 25-2, C). The mesentery is divided perpendicularly to the level of the marginal artery, just proximal to the 1st sigmoidal branch. Unlike in low anterior resection, where extra length is needed for a tension-free colorectal anastomosis, mobilization of the splenic flexure is not required unless the patient is morbidly obese and extra length is needed for stoma construction.
Abdominoperineal Resection
Principles of Preoperative Evaluation
Anatomic Approach to Left Colon Mobilization
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine