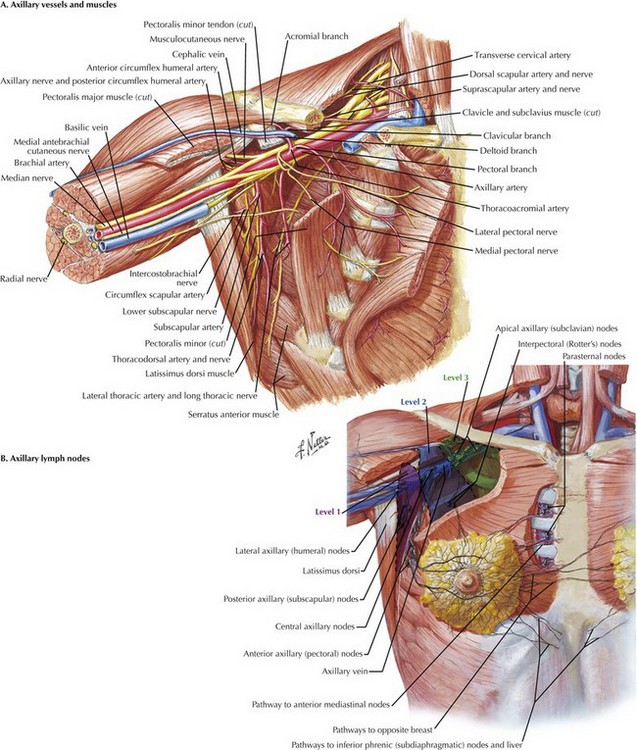
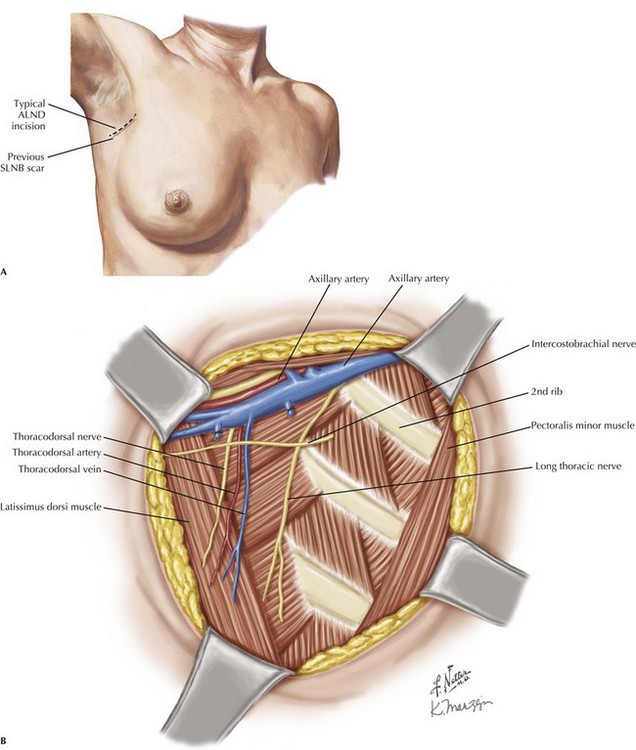
Chapter 49 British surgeon Sir Berkeley Moynihan stated, “Surgery of cancer is not the surgery of the organs; it is the surgery of the lymphatic system.” This statement is especially true of breast cancer and melanoma, in which specific operations are carried out to remove regional lymph node metastases. Lymph node dissection (LND) was the standard of care for staging as well as treating these patients. However, sentinel lymph node biopsy (SLNB) changed the way surgeons stage and treat both breast cancer and melanoma (see Chapter 48). The boundaries of the axilla are the axillary vein superiorly, serratus anterior muscle and chest wall medially, subscapularis and teres minor posteriorly, latissimus dorsi laterally, and pectoralis minor and major muscles anteriorly (Fig. 49-1, A). These structures create a pyramid, with the apex positioned superiorly. The lymph nodes of the axilla are divided into levels I, II, and III, on the basis of their anatomic location in relation to the pectoralis minor (Fig. 49-1, B). Level I nodes are lateral to the lateral edge of the pectoralis minor muscle, level II nodes are posterior to the pectoralis minor, and level III nodes are medial to the medial edge. Lymph nodes are also located between the pectoralis minor and major muscles (Rotter’s interpectoral nodes). The patient should be positioned with the arm abducted 90 degrees. If the patient is undergoing a modified radical mastectomy, access to the axilla is gained through the mastectomy incision (see Chapter 46). Otherwise, a curvilinear incision at the inferior margin of the axillary hairline is typically used (Fig. 49-2, A). If present, a scar from previous SLNB should be used for the incision instead.
Axillary and Inguinal Lymphadenectomy
Introduction
Axillary Lymph Node Dissection
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine