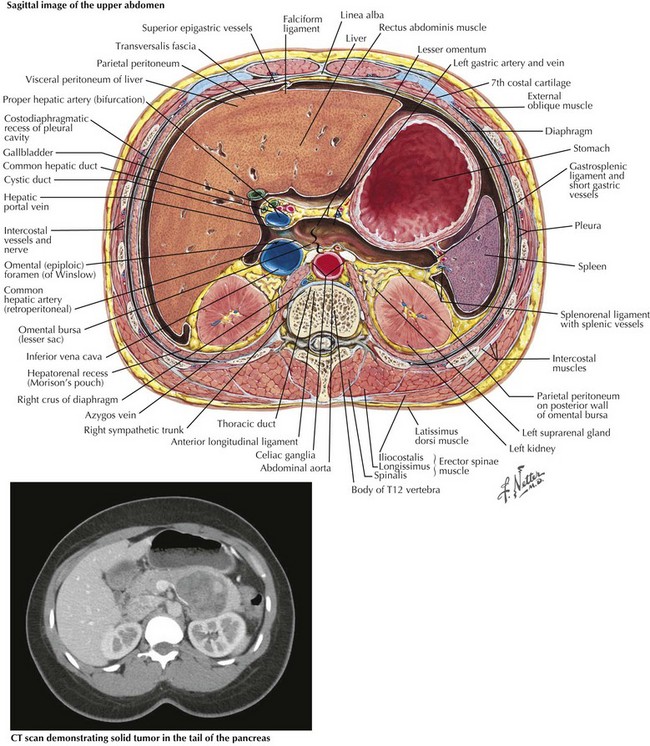
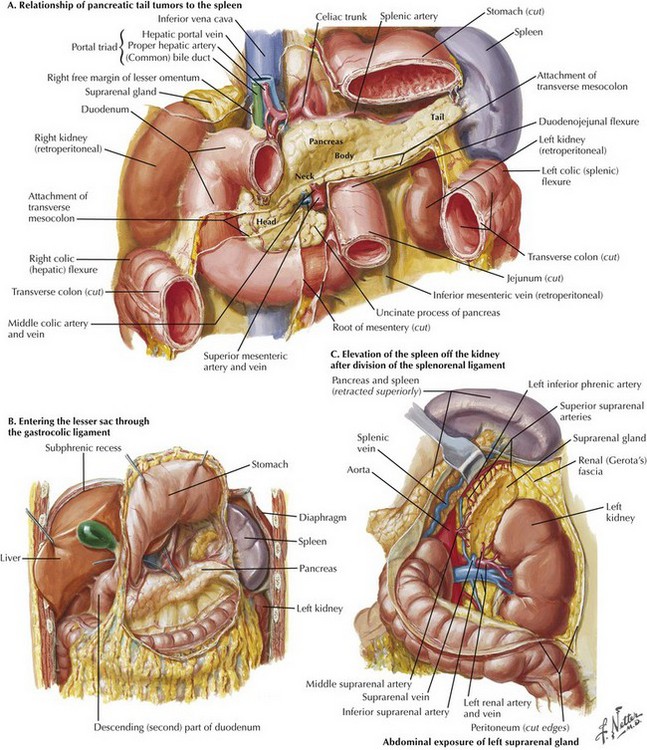
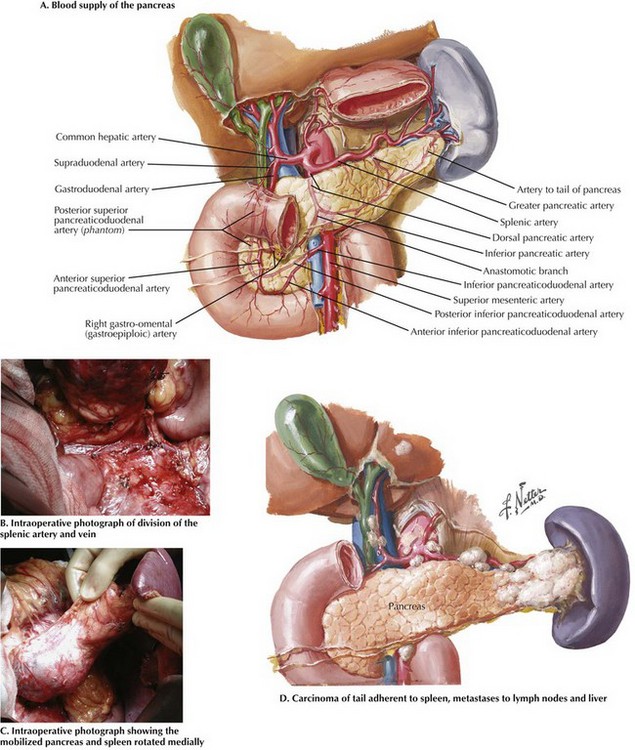
Chapter 15 The indication for distal pancreatectomy will dictate preoperative workup and also influence surgical decision making. Multidetector, dynamic, contrast-enhanced computed tomography (CT) is the preoperative imaging modality of choice for all indications and is essential to surgical planning. CT provides detailed images of the pancreatic pathology and its relationship to surrounding organs, major vasculature, and pancreatic ducts, as well as the presence of metastatic disease (Fig, 15-1). Other modalities, such as endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound (EUS), may also be helpful when a definitive mass is not well visualized. Retrograde distal pancreatectomy with splenectomy is the standard procedure for management of proven or suspected cancers in the body and tail of the pancreas, to ensure the adequacy of the lymph node dissection, or with tumors when the anatomic constraints dictate sacrificing the spleen (Fig. 15-2, A). The pancreas is approached by opening the lesser sac through the gastrocolic ligament below the gastroepiploic vessels (Fig. 15-2, B). The peritoneum overlying the inferior border of the pancreas is divided lateral to the superior mesenteric vessels toward the tail. The splenocolic and splenorenal attachments are divided to mobilize the spleen anteriorly and to the right, separating it from splenic flexure of the colon and from Gerota’s fascia (Fig. 15-2, C). Understanding the vascular anatomy of the pancreas is essential to safe technique (Fig. 15-3, A). The splenic artery is identified at its origin from the celiac trunk and traced distally along the posterosuperior border of the pancreas. It is divided just distal to its origin. The splenic vein is then isolated and divided just proximal to its confluence with the portal vein, preserving the inferior mesenteric vein if possible (Fig. 15-3, B).
Distal Pancreatectomy
Preoperative Evaluation
Surgical Approach
Open Retrograde Distal Pancreatectomy with Splenectomy
Division of Splenic Artery and Vein
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Distal Pancreatectomy