TUMORS WITH ADIPOSE DIFFERENTIATION
4.2 Spindle Cell/Pleomorphic Lipoma
4.5 Atypical Lipomatous Tumor/Well-Differentiated Liposarcoma
4.6 Dedifferentiated Liposarcoma
Lipoma represents the single most common soft tissue tumor of adults. Lipomas tend to increase in prevalence with increasing patient age. They occur in both superficial (subcutaneous) and deep sites. In superficial locations, they present as small, soft, and mobile lesions that are painless. More deep-seated lesions can grow to a much larger size before they are detected clinically. Often they will manifest as increasing size or circumference of an extremity or become noticeable as an asymmetric limb when a patient loses weight. These lesions are clinically benign and are often removed for cosmetic reasons. More deep-seated tumors may recur if incompletely excised.
Conventional lipomas display cytogenetic abnormalities in over half of investigated cases. Some of the most common abnormalities include recombination of 12q13-15 with a variety of partners, aberrations involving 6p21-23, or loss of 13q. There does not appear to be any prognostic significance associated with any of these cytogenetic variations.
HISTOPATHOLOGY
Conventional lipomas resemble mature fat. They are comprised of mature adipose tissue that is virtually indistinguishable from normal fat (Figure 4.1.1). As such, it is often difficult to comment on the “margin” of an excised lipoma. Frequently, lipomas are surrounded by a thin capsule, which may be apparent at the time of excision, but is often not identifiable on microscopy. Lipomas frequently show “degenerative” changes within the central portion of the lesion (Figure 4.1.2). These changes include focal fat necrosis with calcification and/or ossification. Degenerative changes tend to increase with the size and duration of the lesion. Lipomas may also contain a focal myxoid matrix, a feature that can cause some diagnostic confusion (Figure 4.1.3).
Common histologic variants of lipoma include the so-called intramuscular variant, also sometimes referred to as “infiltrating lipoma.” This histologic variant is characterized by intermixed skeletal muscle and adipocytes (Figure 4.1.4). A second common variant represents the angiolipoma. These are characterized by a prominent small vessel proliferation interspersed within the fat (Figure 4.1.5). For some reason, these lesions are frequently multiple and, unlike other lipomas, can be painful. Myolipoma is a lipoma that contains an abundance of smooth muscle (Figures 4.1.6 and 4.1.7). This variant of lipoma occurs most frequently in women and tends to be deep seated. Chondroid lipoma is a rare variant of lipoma containing chondroid matrix material and chondroblasts within an otherwise circumscribed lipoma (Figures 4.1.8 and 4.1.9).
CYTOLOGIC FINDINGS
Aspirates of lipoma are usually hypocellular and composed almost exclusively of intact fragments of fat clinging to either a small fibrous or vascular scaffold. They have a tendency to condense on the slide, forming aggregates that may be difficult to examine cytologically (Figure 4.1.10). In addition, because of the condensation on the slide, the cellular fragments may appear more cellular than one would normally attribute to a benign, relatively paucicellular lesion such as a lipoma (Figure 4.1.11). This represents an artifact of aspiration and should not be confused with a more ominous lesion. Adipocyte nuclei may appear relatively more prominent because of the overall condensation of the lesional tissue. However, clear-cut lipoblasts should not be identified in aspirates.
Occasional confusion may arise when “floret” cells are present in aspirates of the so-called “pleomorphic” variant of lipoma (see Section 4.2). This type of cell is also identified in aspirates of well-differentiated liposarcoma (WDL), but in itself is not diagnostic of this entity. WDL, also known as atypical lipomatous tumor (ALT) depending on location, is the main differential diagnosis for lipoma. These lesions can look similar on cytologic and core biopsy preparations. Ancillary techniques may be needed to exclude a low-grade lipomatous tumor (see Section 4.5).
LIPOMA ARBORESCENS
Lipoma arborescens is sometimes also referred to as synovial lipoma. This process is not a discrete lipoma, but a lipomatous infiltration of the subsynovial soft tissues. Patients tend to be adults and present with symptoms of joint swelling. Histologically, there is expansion of the subsynovial soft tissues with benign-appearing fat (Figure 4.1.12). There is usually also a substantial inflammatory infiltrate.
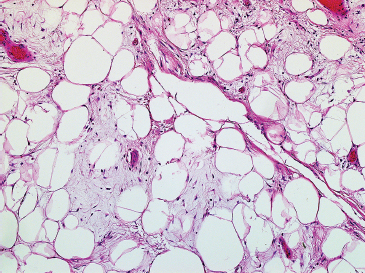
FIGURE 4.1.1 The fat of the lipoma is indistinguishable from normal adipose tissue.
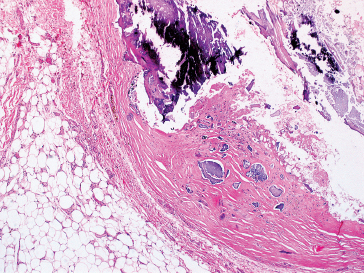
FIGURE 4.1.2 Lipomas frequently show extensive degenerative change. This particular example shows extensive central fat necrosis.
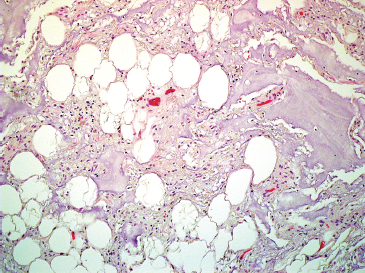
FIGURE 4.1.3 Myxoid change can often be identified within a lipoma. Myxolipomas lack a significant vascular component and lipoblasts (features associated with myxoid liposarcoma).
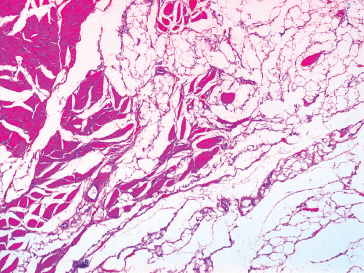
FIGURE 4.1.4 Intramuscular lipomas are often referred to as “infiltrating” lipomas because they appear to be infiltrating between bands of skeletal muscle.
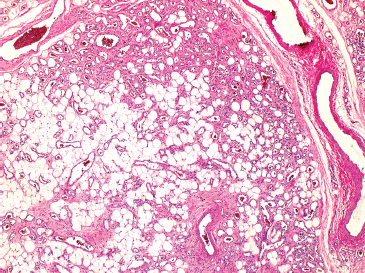
FIGURE 4.1.5 Angiolipomas are characterized by a proliferation of multiple small vessels throughout the lesion. The vascular proliferation tends to be concentrated at the periphery of the lipoma.
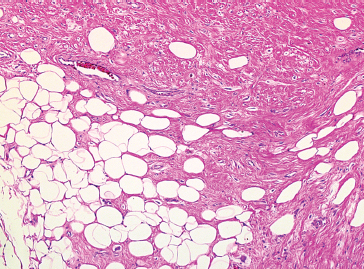
FIGURE 4.1.6 Myolipomas occur most frequently in women. They are comprised of mature fat and smooth muscle.
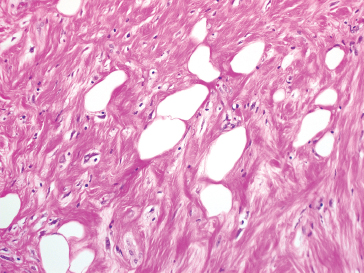
FIGURE 4.1.7 On high power, a myolipoma is identified as a biphasic lesion. Both smooth muscle and fat lack significant cytologic atypia.
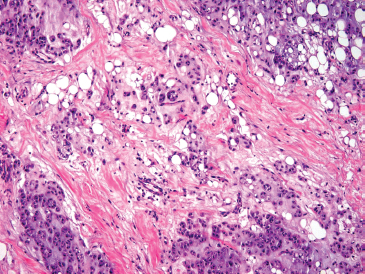
FIGURE 4.1.8 Chondroid lipoma is one of the rarest variants of lipoma. This lesion also tends to occur in women and tends to be deep seated.
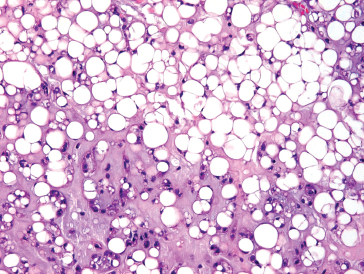
FIGURE 4.1.9 Chondroid lipoma contains a chondromyxoid background as well as a lipoblastic population.
FIGURE 4.1.10 Aspirated normal fat has a tendency to “round up” on slides, making it appear more cellular than it would be if seen in histologic sections.
FIGURE 4.1.11 Because of the condensation phenomenon, normal fat can appear highly cellular and individual adipocytes can simulate the appearance of lipoblasts.
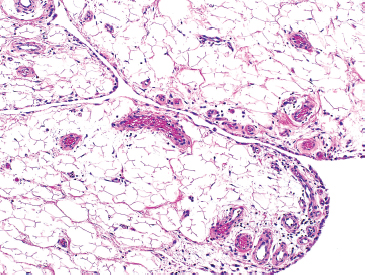
FIGURE 4.1.12 Lipoma arborescens is an infiltration of the synovial soft tissue with fat. This gives rise to a hyperplastic “villous”-appearing synovium.
4.2 Spindle Cell/Pleomorphic Lipoma
Spindle cell lipoma is a variant of lipoma that deserves special mention because of its unique clinical, histologic, and immunohistochemical features. This is a circumscribed lesion, which frequently presents in the trunk, neck, or shoulders of middle-aged to elderly men, median age of 55 years. About 10% of all cases occur in adult women. Spindle cell/pleomorphic lipoma is unlikely to occur in a child or adolescent. Spindle cell/pleomorphic lipomas may be confused with more aggressive lesions due to the overall cellularity of the neoplasm. This lesion is completely benign and can be cured with a simple excision.
Spindle cell lipoma is closely related to pleomorphic lipoma, a lesion that can show striking histologic irregularities. Many of these lesions tend to show mixed features, and they probably represent a histologic continuum of findings. Pleomorphic lipoma shows a similar site distribution as spindle cell lipoma.
HISTOPATHOLOGY
As the name implies, spindle cell lipomas are comprised of a relatively dense population of spindled cells with a less prominent adipocytic component. The spindled cells are very small and are usually arranged in a very dense, frequently parallel array. They have monotonous, ovoid nuclei with indistinct cytoplasm (Figure 4.2.1). The background matrix material usually has a myxoid appearance. Mitotic activity is low, and mast cells may be identified. The fat of spindle cell lipomas is mature; there should be no true lipoblasts. In hybrid spindle cell/pleomorphic tumors, there may be small “pseudo-lipoblast-like” cells (Figure 4.2.2). Spindle cells lipomas also typically contain a variable number of thick ropey collagen bundles as well as rare multinucleate floret-type cells. When floret-type multinucleate cells predominate, the lesion is probably best termed pleomorphic lipoma (Figure 4.2.3). The floret cells of pleomorphic lipoma are very similar to those sometimes identified in association with atypical lipomatous tumor (ALT)/well differentiated liposarcoma (WDL).
One key diagnostic feature of spindle cell lipoma is its immunoreactivity for the CD34 antigen. Reactivity is strong and diffuse throughout the lesion and is helpful for discriminating this benign lesion from other more cellular tumors, including ALT (Figure 4.2.4).
CYTOLOGIC FINDINGS
Aspirates of spindle cell lipoma tend to be more cellular than other variants of lipoma. They frequently are comprised of background matrix material and mature-appearing adipocytes. Fragments of ropey collagen as well as a small bland spindle cell population are key diagnostic features (Figure 4.2.5). Aspirates of pleomorphic lipoma may contain floret cells (Figure 4.2.6). This feature can easily cause diagnostic confusion.
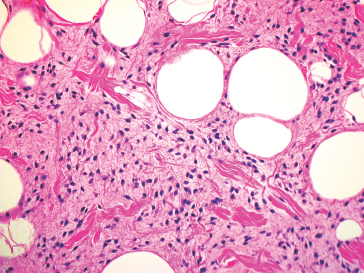
FIGURE 4.2.1 A spindle cell lipoma containing adipose, small spindled cells and fragments of ropey collagen.
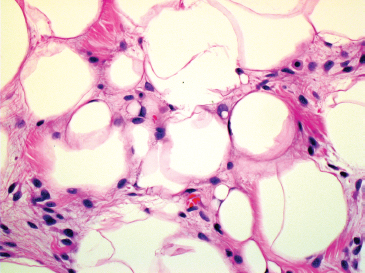
FIGURE 4.2.2 Small pseudo-lipoblasts are often identified in the spindle cell variant of lipoma.
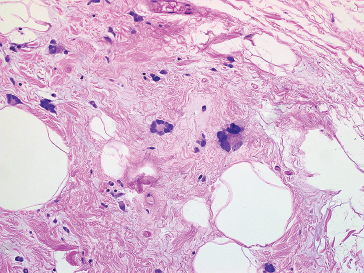
FIGURE 4.2.3 Multinucleate “floret”-type cells are seen in association with pleomorphic lipoma.
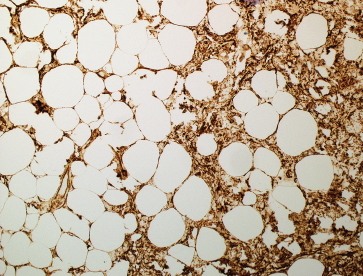
FIGURE 4.2.4 Immunohistochemical staining for CD34 is diffusely and strongly positive within spindle cell lipoma.
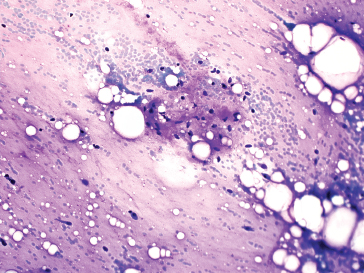
FIGURE 4.2.5 Aspirates of spindle cell lipoma usually have prominent myxoid material in the background. They also contain fat vacuoles and small spindled cells.
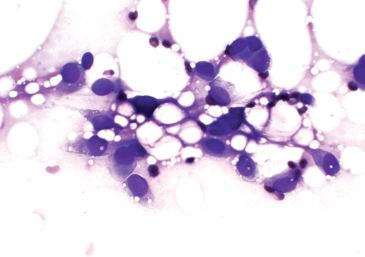
FIGURE 4.2.6 Aspirates of pleomorphic lipoma may have large nuclei and multinucleate cells.
Hibernoma is an unusual benign neoplasm that is thought to be a morpohologic variant of a benign lipoma. It is composed of so-called “brown fat,” which is normally identified in newborns and hibernating animals. In infants, about 5% of body fat is of the “brown” variety. It is normally distributed along the upper back region and is thought to provide a survival advantage for infants who are susceptible to cold. In human adults, the distribution of brown fat is very limited (cervical, upper chest, and axillary regions). The brown descriptor applies to the gross appearance of the lesion, often a darker yellow to brown color on examination. Microscopically, brown fat differs from normal “white” fat in its overall vascularity, numerous mitochondria, and the presence of microvesicular lipid instead of the single lipid vacuole of regular fat.
Hibernomas occur in a wide age range of individuals with a peak incidence in younger adults. The most common locations for hibernomas include the extremities, particularly the thigh, as well as the head, neck, and trunk. Rare examples of deep-seated hibernoma (retroperitoneal, intra-abdominal) have been reported in addition to rare intraosseous tumors. A hibernoma is most often subcutaneous or intramuscular and presents as a slow-growing, painless mass. Hibernomas are completely benign tumors with no potential for recurrence, metastasis, or malignant transformation. Of special note, hibernomas have been reported to be the cause of false-positive diagnoses of malignancy on positron emission tomography-computed tomography (PET-CT) scans. Because of their abundant mitochondria, hibernomas are metabolically active, leading to a “hot” or glucose-avid signal on PET.
Molecular studies have demonstrated complex structural rearrangements of the 11q13 region. Recently it has been discovered that these aberrant gene rearrangements involve deletions of tumor suppressor genes including the MEN1 gene.
HISTOPATHOLOGY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


