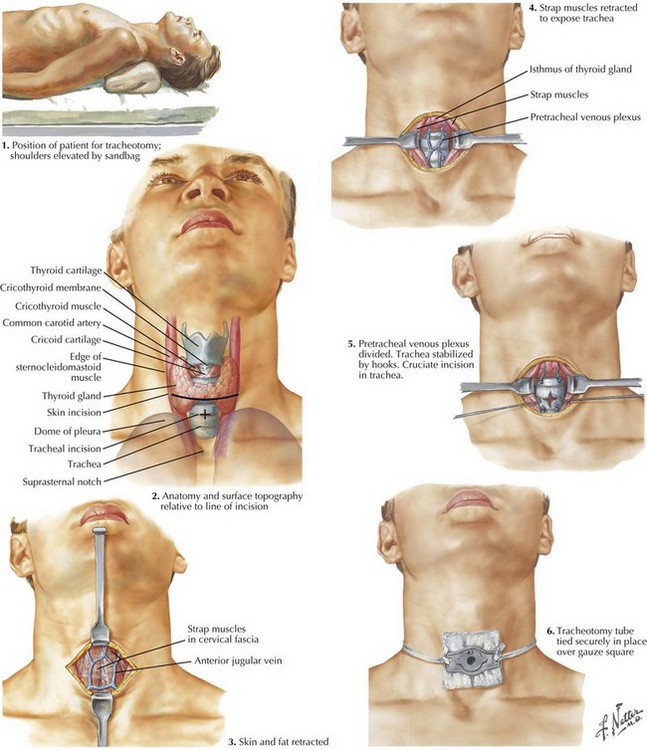
Chapter 2 The patient is placed in the supine position. The surgeon might consider placing the neck into slight extension, but this should not be too far past the neutral position, so that the skin incision remains in line with the tracheal incision. A shoulder roll may be used in some patients to assist with positioning (Fig. 2-1). The thyroid notch superiorly, cricoid cartilage, and suprasternal notch inferiorly can usually be palpated and should be marked (Fig. 2-1). If an awake tracheotomy is being performed, the skin is injected with 1% lidocaine with 1 : 100,000 epinephrine solution for hemostasis and anesthesia. According to surgeon preference, this injection may also be done for general anesthesia patients. A vertical or horizontal incision is made in the midline of the neck, about 2 cm above the sternal notch, and is carried down until the strap muscles are visible.
Tracheotomy and Cricothyrotomy

Surgical Anatomy and Tracheotomy Procedure
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Basicmedical Key
Fastest Basicmedical Insight Engine