Chapter 2 The Thorax
Xiphisternal joint marks inferior border of heart and superior border of liver.
A traumatic sternal fracture requires evaluation for heart injury.
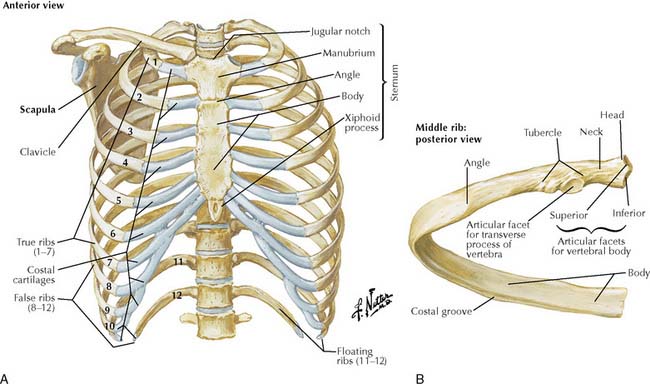
TABLE 2-1 Joints of Thoracic Wall
| Joint | Articulating Structures | Comments |
|---|---|---|
| Manubriosternal | Manubrium with body of sternum | Sternal angle marks level of second costal cartilage |
| Costochondral | Rib with costal cartilage | |
| Sternocostal | Costal cartilages 1-7 with sternum |
Dimpling and an orange peel appearance of the skin and nipple retraction are signs of breast cancer.
Klinefelter syndrome males have an increased incidence of breast cancer.
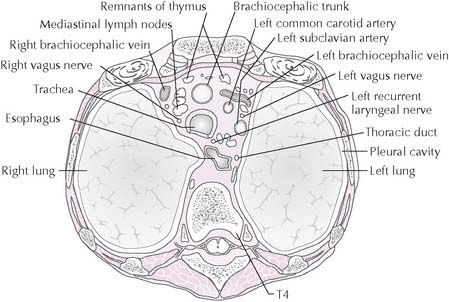
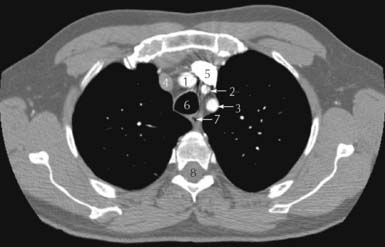
2-4 Axial CT near same level as Figure 2-3. Brachiocephalic trunk = 1; left common carotid artery = 2; left subclavian artery = 3; right brachiocephalic vein = 4; left brachiocephalic vein = 5; trachea = 6; esophagus = 7; spinal cord = 8.
(From Weir, J, Abrahams, P: Imaging Atlas of Human Anatomy, 3rd ed. London, Mosby Ltd., 2003, p 92, b.)
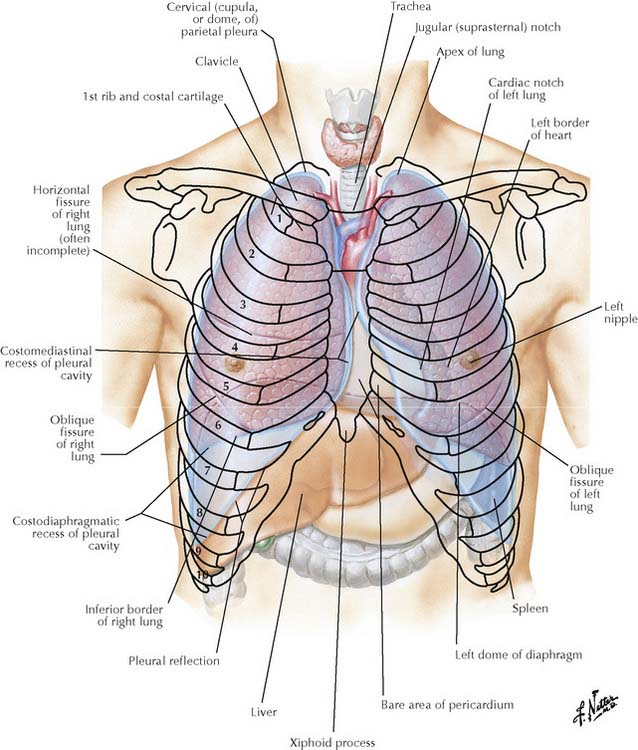
2-5 Surface projections of lungs and pleurae. Numbers, ribs.
(From Netter, F H: Atlas of Human Anatomy, 4th ed. Philadelphia, Saunders, 2006, Plate 196.)
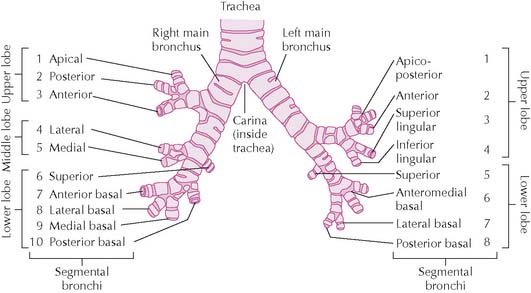
Bronchopulmonary segments are independent functional and surgical units.
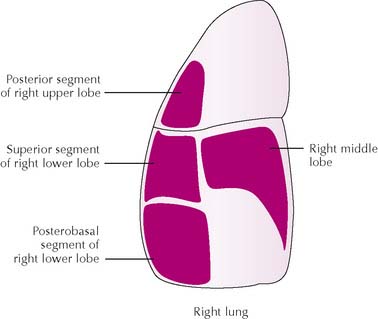
Patient position determines the location of inhaled foreign objects.
Gravity moves foreign material to different bronchopulmonary segments of the right lung depending on the patient’s position (Figure 2-8). In a standing or sitting patient, the posterobasal segment is involved; in the supine patient, the superior segment of the lower lobe; in the right-sided recumbent position, the middle lobe or posterior segment of the right upper lobe. The arrangement of segments also means that a patient can be optimally positioned for postural drainage of an infected bronchopulmonary segment aided by percussion of the chest wall over the segment.
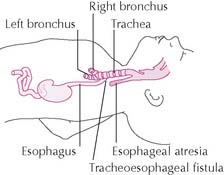
A congenital tracheoesophageal fistula is an abnormal communication between the trachea and distal esophagus usually associated with esophageal atresia (blind-ending esophagus) (Figure 2-9). The resulting regurgitation and aspiration of swallowed milk (and possible reflux of gastric contents into lungs) cause pneumonia. Because esophageal atresia prevents the fetus from swallowing and absorbing amniotic fluid in the small intestine, the condition is often accompanied by excess amniotic fluid (polyhydramnios). An acquired tracheoesophageal fistula may result from malignancy, infection, or trauma.
Patient with dyspnea may lean on upper extremities to allow accessory muscles to aid in respiration.
Tension pneumothorax is a life-threatening condition in which air enters the pleural cavity during inspiration due to a penetrating wound but cannot exit during expiration. Air pressure increases on the affected side, and the mediastinum shifts away, compressing the contralateral lung and compromising venous return to the heart (Figure 2-10). Bedside ultrasonography often replaces chest radiographs for diagnosis. The patient complains of chest pain and dyspnea. Jugular venous distention and a tracheal shift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


