Fig. 16.1 Cross-section of muscle.
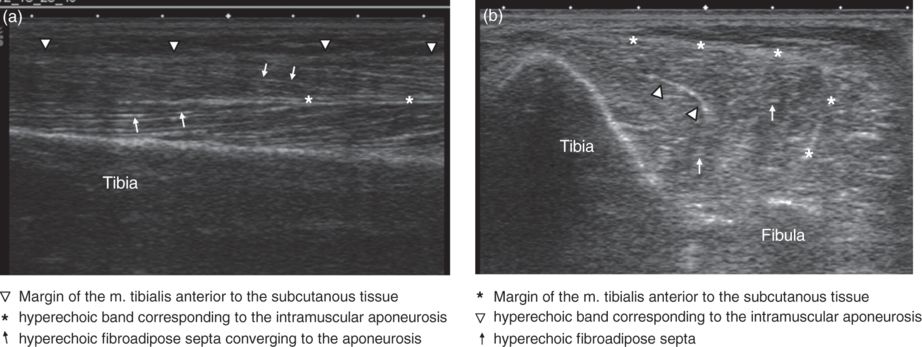
Fig. 16.2 Ultrasound of skeletal muscle. Longitudinal (a) and transverse (b) scans.
Patient preparation
The patient should be placed as comfortable as possible and in a way that the target muscle can be reached without major difficulties. Standard disinfectant fluid can be used as the contact medium. Alternatively, before performing the ultrasound, standard skin disinfection can be performed and the injection carried out through the standard bacteriostatic gel (Berweck and Heinen, 2005).
Ultrasound-guided injection technique
The target muscle is identified and scanned by ultrasound in the longitudinal and transverse planes. The optimum injection area is located where most of the motor endplates are assumed to be (Campenhout and Molenaers, 2011).
There are two ways to place the needle with ultrasound guidance.
- Indirect technique.
The puncture site is marked by ultrasound and the depth of the target region is measured. The needle is then placed blindly perpendicular to the skin surface and as deep as measured before. There is no real-time control of the injection itself.
- Real-time technique.
The target region is shown by ultrasound and the needle is advanced under direct ultrasound control. This technique is preferred.
The muscle can be viewed in a longitudinal or transverse plane. The transverse projection allows the differentiation of structures in the neighborhood and the identification of the muscles based on their characteristic pattern. This is especially helpful when injecting smaller muscles such as those of the upper extremity. For iliopsoas injection, the longitudinal view is favored.
For the injection, two basically different approaches are described: needle parallel to the long axis of the probe and needle perpendicular to the long axis of the probe.
Needle parallel to the long axis of the probe
The needle is inserted approximately 1 to 2 cm distal to the probe and advanced under real-time control in the longitudinal axis of the probe (Fig. 16.3); the advancement of the needle can be followed as a hyperechoic line. The higher the injection angle relative to the ultrasound beam, the better the visualization of the needle. If the needle advancement cannot be followed directly, the position can be estimated indirectly by imaging the movements of the surrounding soft tissues during real-time observation. After correct placement and control aspiration, BoNT is injected under real-time observation mode. The solution of BoNT in saline presents mostly as a hyperechoic area within the muscle, sometimes with a dorsal echo-extinction. By changing the position of the needle, the BoNT can be well distributed in the muscle belly.
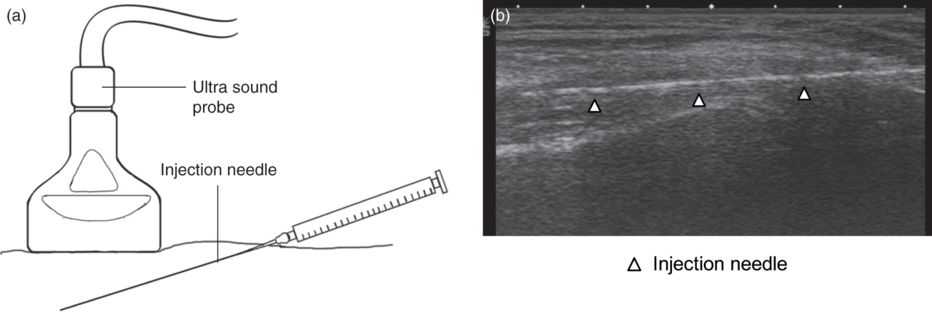
Fig. 16.3 Injection technique with the needle parallel to the long axis of the probe. (a) The relationship of the probe to the needle. (b) Ultrasound view with the arrowheads indicating the position of the needle.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


